
Abstract
Erectile dysfunction (ED) is a common condition in men with cardiovascular disease (CVD), yet it is frequently under-recognized and under-diagnosed in clinical practice. Men are often reluctant to seek treatment, even though they have lower sexual and overall life satisfaction compared with healthy people. Moreover, moderate ED has a similar impact on a patient's satisfaction with sexual life as severe ED. Both patient- and physician-related factors contribute to the under-diagnosis and under-recognition of ED. A holistic, patient-centered approach is fundamental to the management of ED in men with CVD. Sexual medical training courses can enhance physicians' communication skills. Implementing lifestyle changes, recognizing the factors that lead to poor compliance and reducing psychologic stress can also lead to improvements in the management of ED. As ED and CVD share similar risk factors, a common prevention strategy has been proposed.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 8 print issues and online access
$259.00 per year
only $32.38 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
McKinlay JB . The worldwide prevalence and epidemiology of erectile dysfunction. Int J Impot Res 2000; 12 (Suppl 4): S6–S11.
Chiurlia E, D’Amico R, Ratti C, Granata AR, Romagnoli R, Modena MG . Subclinical coronary artery atherosclerosis in patients with erectile dysfunction. J Am Coll Cardiol 2005; 46: 1503–1506.
Jackson G, Padley S . Erectile dysfunction and silent coronary artery disease: abnormal computed tomography coronary angiogram in the presence of normal exercise ECGs. Int J Clin Pract 2008; 62: 973–976.
Haro JM, Beardsworth A, Casariego J, Gavart S, Hatzichristou D, Martin-Morales A et al. Treatment-seeking behavior of erectile dysfunction patients in Europe: results of the Erectile Dysfunction Observational Study. J Sex Med 2006; 3: 530–540.
Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, McKinlay JB . Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts Male Aging Study. J Urol 2000; 163: 460–463.
Carson CC, Lue TF . Phosphodiesterase type 5 inhibitors for erectile dysfunction. BJU Int 2005; 96: 257–280.
Brant WO, Bella AJ, Lue TF . Treatment options for erectile dysfunction. Endocrinol Metab Clin North Am 2007; 36: 465–479.
Beckman TJ, Abu-Lebdeh HS, Mynderse LA . Evaluation and medical management of erectile dysfunction. Mayo Clin Proc 2006; 83: 385–390.
Hatzichristou D, Haro JM, Martin-Morales A, von Keitz A, Riley A, Bertsch J et al. Patterns of switching phosphodiesterase type 5 inhibitors in the treatment of erectile dysfunction: results from the Erectile Dysfunction Observational Study. Int J Clin Pract 2007; 61: 1850–1862.
Papaharitou S, Athanasiadis L, Nakopoulou E, Kirana P, Portseli A, Iraklidou M et al. Erectile dysfunction and premature ejaculation are the most frequently self-reported sexual concerns: profiles of 9536 men calling a helpline. Eur Urol 2006; 49: 557–563.
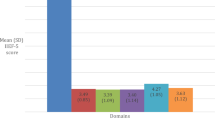
Mallis D, Moisidis K, Kirana P-S, Papaharitou S, Simos G, Hatzichristou D . Moderate and severe erectile dysfunction equally affects life satisfaction. J Sex Med 2006; 3: 442–449.
Papaharitou S, Nakopoulou E, Kirana P, Iraklidou M, Athanasiadis L, Hatzichristou D . Women's sexual concerns: data analysis from a help-line. J Sex Med 2005; 2: 652–657.
World Health Organization. Sexual health. http://www.who.int/reproductive-health/gender/sexualhealth.html. (Accessed on 16 April 2008).
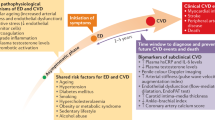
Hatzichristou D, Tsimtsiou Z . Prevention and management of cardiovascular disease and erectile dysfunction: toward a common patient-centered, care model. Am J Cardiol 2005; 96 (Suppl): 80M–84M.
Hatzichristou D, Rosen RC, Broderick G, Clayton A, Cuzin B, Derogastis L et al. Clinical evaluation and management strategy for sexual dysfunction in men and women. J Sex Med 2004; 1: 49–57.
Hatzimouratidis K, Hatzichristou DG . A comparative review of the options for treatment of erectile dysfunction: which treatment for which patient? Drugs 2005; 65: 1621–1650.
Tsimtsiou Z, Hatzimouratidis K, Nakopoulou E, Kyrana E, Salpigidis G, Hatzichristou D . Predictors of physicians’ involvement in addressing sexual health issues. J Sex Med 2006; 3: 583–588.
Athanasiadis L, Papaharitou S, Salpiggidis G, Tsimtsiou Z, Nakopoulou E, Kirana P-S et al. Educating physicians to treat erectile dysfunction patients: developments and evaluation of a course on communications and management strategies. J Sex Med 2006; 3: 47–55.
Kostis JB, Jackson G, Rosen R, Barrett-Connor E, Billups K, Burnette AL et al. Sexual dysfunction and cardiac risk (the Second Princeton Consensus Conference). Am J Cardiol 2005; 96: 313–321.
Derby CA, Mohr BA, Goldstein I, Feldman HA, Johannes CB, McKinlay JB . Modifiable risk factors and erectile dysfunction: can lifestyle changes modify risk? Urology 2000; 56: 302–306.
Nied RJ, Franklin B . Promoting and prescribing exercise for the elderly. Am Fam Physician 2002; 65: 419–426.
Morris LS, Schulz RM . Patient compliance–an overview. J Clin Pharm Ther 1992; 17: 283–295.
Hansson L . Why don’t you do as I tell you?’ Compliance and antihypertensive regimens. Int J Clin Pract 2002; 56: 191–196.
Wang PS, Bohn RL, Knight E, Glynn RJ, Mogun H, Avorn J . Noncompliance with antihypertensive medications. The impact of depressive symptoms and psychological factors. J Gen Intern Med 2002; 17: 504–511.
Romanelli J, Fauerbach JA, Bush DE, Ziegelstein RC . The significance of depression in older patients after myocardial infarction. J Am Geriatr Soc 2002; 50: 817–822.
Goldstein I . The mutual reinforcing triad of depressive symptoms, cardiovascular disease, and erectile dysfunction. Am J Cardiol 2000; 86 (Suppl): 41F–45F.
Torpy JM, Lynm C, Glass RM . Chronic stress and the heart. JAMA 2007; 298: 1722.
Denollet J, Vaes J, Brutsaert DL . Inadequate response to treatment in coronary heart disease. Adverse effects of type D personality and younger age on 5-year prognosis and quality of life. Circulation 2000; 102: 630–635.
Institute of Medicine (IOM), Committee on Health Care in America. Crossing the Quality Chasm: a New Health System for the 21st Century. National Academy Press: Washington, DC, USA, 2001.
Cioffi D . Beyond attentional strategies: a cognitive–perceptual model of somatic interpretation. Psychol Bulletin 1991; 109: 25–41.
Acknowledgements
I acknowledge medical writing support by Vicky Hinstridge (a Senior Medical Writer contracted to GCC) and Jackie Phillipson of Gardiner-Caldwell Communications; this support was funded by Eli Lilly and Company. Diane Stothard (Eli Lilly and Company) provided support by reviewing this paper.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure
D Hatzichristou is involved in FDA/EMEA approved clinical trials for Eli Lilly, Bayer, and Pfizer and is also a speaker for Astellas Pharma Inc., Bayer, Eli Lilly and Company, Pfizer, and Sanofi-Aventis.
Rights and permissions
About this article
Cite this article
Hatzichristou, D. Understanding individuals' response to erectile dysfunction. Int J Impot Res 20 (Suppl 2), S15–S20 (2008). https://doi.org/10.1038/ijir.2008.48
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijir.2008.48
This article is cited by
-
Raising awareness for the diagnosis and treatment of erectile dysfunction in patients with high risk to develop ED
International Journal of Impotence Research (2009)
