
Abstract
To investigate if children who later developed acute lymphoblastic leukaemia (ALL) were prenatally infected with HHV-6 and/or EBV, Guthrie cards taken at birth were analysed by PCR. Guthrie cards from 54 patients with ALL and 47 healthy controls matched for age and birth place were tested negative for both HHV-6 and EBV DNA. All samples contained amplifiable DNA when tested by HLA-DQ PCR. Our negative findings suggest that childhood ALL is unlikely to be associated with an in utero infection with EBV or HHV-6.
Similar content being viewed by others

Main
Acute lymphoblastic leukaemia (ALL) is the most frequent childhood malignancy in Western countries. The different subtypes of leukaemia differ in their patterns of genetic change, natural history, prognosis and possibly aetiology (Doll, 1989; Ross, 1999). One model for the aetiology of ALL is prenatal infection and such a maternal infection could affect foetal haematopoiesis early in the liver and later in the bone marrow (Ohls and Christensen, 2000). The relevant agent would have to cross the placenta, induce genomic instability in the lymphocytes and infect the foetus without causing severe foetal abnormalities (Smith, 1997). We have analysed human polyomaviruses (JCV and BKV) and human parvovirus B19 in Guthrie cards from children who later developed ALL, but could detect neither polyomavirus DNA nor parvovirus DNA from ALL cases or controls (Priftakis et al, 2003; Isa et al, 2004).
Epstein–Barr virus (EBV) and human herpes virus 6 (HHV-6) are two potentially oncogenic viruses, widely distributed in the human population, which can be spread by vertical or horizontal (in utero) transmission. Since they persist and establish latency in their natural host after primary infection, they may be reactivated during immunosuppression (Matsuda et al, 1999). The viral latency is primarily established in lymphocytes, which may be important in relation to childhood ALL (Gustafsson et al, 2000; Salonen et al, 2002).
Our study was conducted to determine if a group of children with ALL were prenatally infected with HHV-6 or EBV. Guthrie cards taken at birth were collected and analysed for the presence of these viruses.
Patients and methods
Patients
We collected Guthrie cards from 54 children who had developed ALL. In all, 50 of these children had been diagnosed as pre-B ALL (either CD10+, CD20+, FAB L1 or L2) and four children were diagnosed as T-ALLs (CD3+ or CD8+). A total of 24 children were diagnosed before the age of 4, 16 children were between 5 and 9 years, 12 children were between 10 and 14 years of age and two children were older than 14 years. The median age at diagnosis was 5 years (range 9 months–17 years, mean 5.9 years). These children had been admitted for treatment at four different Paediatric Oncology Swedish Centres from 1980 through 2001. As a control group, we obtained 47 healthy controls that were matched for age and birthplace, and data from the controls were collected from the Swedish Medical Birth Register, which is a standardised set of medical records introduced in Sweden in 1973 (Cnattingius et al, 1990). The capillary blood from both groups is collected at 3–5 days of age. After the screening analysis, the Guthrie cards are stored at 4°C at the PKU laboratory, at Karolinska University Hospital, Huddinge.
Two bone marrow-transplanted patients were positive for HHV-6 and EBV-DNA, respectively. These two patients were included as positive controls. Guthrie cards ‘spiked’ with blood from these patients were tested for the presence of HHV-6 or EBV DNA. Blood samples were taken from these two patients and added to a new Guthrie card.
Methods
DNA extraction by minimal essential medium (MEM)
At the time of analysis, the filter paper samples were stored at room temperature before extraction. The extraction method utilised was MEM extraction, previously described, with minor modifications (Barbi et al, 1996). Three uniform discs 3 mm in diameter, were removed from the filter paper, and prepared using special precautions in order to avoid contamination, as previously described.
HHV-6 DNA detection
Presence of HHV-6 DNA was analysed by a nested PCR, with the primers corresponding to the conserved region of HHV-6 of both variants A and B amplifying a 173 bp segment (Wang et al, 1996). Purified DNA extracted from HHV-6 strain GS (type A) and strain Z29 (type B) were used as positive controls in all PCRs. The sensitivity estimated using known concentrations of positive controls DNA was 20–30 genomes per PCR reaction for both strains (Wang et al, 1996).
EBV DNA detection
Presence of EBV DNA was analysed by a nested PCR with the primers corresponding to the fragment of EBV EBNA gene 1 amplifying a 208 bp segment (Cinque et al, 1993; Wang et al, 1996).
HLA PCR
As a control for the presence of DNA extracted from Guthrie cards and for DNA amplifiability, a PCR with a set of HLA DQ primers was performed (Saiki et al, 1986). The HLA PCR-negative samples were not used for further investigation.
Ethical considerations
Written informed consent was obtained from patients, controls and parents. The local ethics committee of the Karolinska Institutet at Karolinska University Hospital approved the study protocol.
Results and discussion
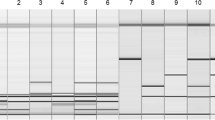
The Guthrie cards of all 54 patients with ALL, as well as all 47 healthy controls, were tested negative by PCR for both HHV-6 DNA and EBV DNA. All samples contained amplifiable DNA when tested by HLA-DQ PCR. HHV-6 or EBV DNA could be detected in the blood as well as in the ‘spiked’ Guthrie cards from the two BMT patients with HHV-6 and EBV infection, respectively.
The use of stored Guthrie cards as a source of DNA has been shown to have several uses. DNA is relatively stable and blood collected from newborns contains 2–3 times higher levels of nucleic acid when compared to adults. In several studies, it has been shown that viral DNA could be successfully amplified from Guthrie cards in case of congenital CMV, HSV and HIV infection (Cassol et al, 1991; Barbi et al, 1996; Fischler et al, 1999).
The difficulty to divide childhood leukaemia into homogenous subgroups may explain the complexity when investigating different aetiological factors. In our material, the majority of children had pre-B-ALL. It has been suggested that infection in utero with a virus that has the oncogenic potential could be involved in the initiation of ALL, by inducing genomic instability and allowing specific effects on B lymphocytes. Twin studies suggest that an additional molecular event or exposure is then required postnatally for the preleukaemic clone to expand. The second event, leading to leukaemia, can occur at a time of maximum stress on lymphocyte precursor proliferation and may be promoted by exposure to a common infectious agent (Gale et al, 1997; Greaves, 1999; Wiemels et al, 1999).
Space–time clustering of ALL has raised the possibility of an infectious agent in ALL. Kinlen and others proposed that the mixing of previously separate groups of people, as in the creation of new towns in rural construction projects or military camps, may raise the incidence of leukaemia by facilitating transmission of infective agents (Kinlen et al, 1990; Kinlen and Balkwill, 2001; Kinlen et al, 2002). Although most reports have emphasized space–time clustering at diagnosis (Petridou et al, 1996; Alexander et al, 1997; Gilman et al, 1999), recent studies have detected space–time clustering around the time of birth (Alexander, 1992; Gustafsson and Carstensen, 1999, 2000; Birch et al, 2000). This could implicate that events or exposures might originate in utero. But there are also opportunities for leukaemogenic infection to occur after birth and before the children in space–time clustering studies have moved away from birth addresses.
Another model for virus transmission during pregnancy is suggested by observations that leukaemia in cats can result from maternal transmission (Knox et al, 1980).
Intrauterine infection is a result of either primary maternal infection or reactivation of the latent infection. Primary infection with HHV-6 during pregnancy is a rare event, since more than 90% are seropositive at the age of 3, infection being most frequent during the first year of life (Dahl et al, 1990, 1999; Hall et al, 1994). HHV-6 reactivation may be more common when foetal transmission may occur in approx. 1% of pregnancies (Dahl et al, 1999). HHV-6 was first isolated from cultures of the peripheral blood lymphocytes of patients with AIDS and lymphoproliferative diseases; it is considered to play an important role in the development of complications after stem cell transplantation (Salahuddin et al, 1986; Matsuda et al, 1999). EBV was first discovered through its close relationship with the endemic form of Burkitt lymphoma, the most common childhood cancer in equatorial Africa (Burkitt, 1958; Epstein et al, 1964). EBV reactivation is also frequent in organ and stem cell transplant patients in whom it can produce lethal lymphoproliferative disease (Gustafsson et al, 2000). The experience of EBV in the transplant setting clearly illustrates the ability of the EBV virus to reactivate during immunosuppression and its oncological potential. Besides the transplant setting, EBV is also frequently reactivated during pregnancy (Costa et al, 1985). The seroprevalence of EBV in adults has been reported to be higher than 90% (Rickinson, 1996). In a recent published study (Lehtinen et al, 2003), it was shown that maternal reactivation of EBV infection during the first trimester was associated with a significant increased risk of developing ALL in the offspring. Maternal infection was determined by detection of EBV-specific IgM antibodies in the serum. As it is known, the specificity of IgM is not so good regarding EBV reactivation as compared to determining primary EBV infection, so PCR analysis was performed in addition (Lehtinen et al, 2003). Of 77 IgM positive women, there were only two that were EBV DNA positive, compared to three cases of EBV DNA-positive women in the control group, indicating that viremia was not often established during reactivation (Lehtinen et al, 2003).
The fact that neither HHV-6 DNA nor EBV were detected in dried blood spots obtained from newborns at birth indicates that congenital infections with these viruses are uncommon. The possibility of false-negative results due to infection early in pregnancy and being latent at birth must be considered. However, for congenital CMV infection, it has been shown that Guthrie cards were positive for CMV DNA even when the maternal infection took place during the first or second trimester, indicating that viremia persisted to birth (Peckham, 1991). Similar findings were reported in cases of intrauterine foetal death in association with parvovirus B19 infection (Tolfvenstam et al, 2001).
HHV-6 DNA and EBV-DNA were neither detected by PCR in blood from Guthrie cards in children who had developed ALL nor from healthy controls. Hence, it is unlikely that childhood ALL is associated with an in utero infection with these viruses although a latent infection cannot be ruled out by this method, nor infection after birth. In view of the epidemiological evidence for a relation between childhood ALL and infection, the search for a virus aetiology must continue.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Alexander FE (1992) Space–time clustering of childhood acute lymphoblastic leukaemia: indirect evidence for a transmissible agent. Br J Cancer 65: 589–592
Alexander FE, Chan LC, Lam TH, Yuen P, Leung NK, Ha SY, Yuen HL, Li CK, Lau YL, Greaves MF (1997) Clustering of childhood leukaemia in Hong Kong: association with the childhood peak and common acute lymphoblastic leukaemia and with population mixing. Br J Cancer 75: 457–463
Barbi M, Binda S, Primache V, Novelli C (1996) Cytomegalovirus in peripheral blood leukocytes of infants with congenital or postnatal infection. Pediatr Infect Dis J 15: 898–903
Birch JM, Alexander FE, Blair V, Eden OB, Taylor GM, McNally RJ (2000) Space–time clustering patterns in childhood leukaemia support a role for infection. Br J Cancer 82: 1571–1576
Burkitt D (1958) A sarcoma involving the jaws in African children. Br J Surg 46: 218–223
Cassol S, Salas T, Arella M, Neumann P, Schechter MT, O'Shaughnessy M (1991) Use of dried blood spot specimens in the detection of human immunodeficiency virus type 1 by the polymerase chain reaction. J Clin Microbiol 29: 667–671
Cinque P, Brytting M, Vago L, Castagna A, Parravicini C, Zanchetta N, D'Arminio Monforte A, Wahren B, Lazzarin A, Linde A (1993) Epstein–Barr virus DNA in cerebrospinal fluid from patients with AIDS-related primary lymphoma of the central nervous system. Lancet 342: 398–401
Cnattingius S, Ericson A, Gunnarskog J, Kallen B (1990) A quality study of a medical birth registry. Scand J Soc Med 18: 143–148
Costa S, Barrasso R, Terzano P, Zerbini M, Carpi C, Musiani M (1985) Detection of active Epstein–Barr infection in pregnant women. Eur J Clin Microbiol 4: 335–336
Dahl H, Fjaertoft G, Norsted T, Wang FZ, Mousavi-Jazi M, Linde A (1999) Reactivation of human herpesvirus 6 during pregnancy. J Infect Dis 180: 2035–2038
Dahl H, Linde A, Sundqvist VA, Wahren B (1990) An enzyme-linked immunosorbent assay for IgG antibodies to human herpes virus 6. J Virol Methods 29: 313–323
Doll R (1989) The epidemiology of childhood leukemia. J R Stat Soc Series 152: 341–351
Epstein MA, Achong BG, Barr YM (1964) Virus particles in cultured lymphoblasts from Burkitt's lymphoma. Lancet 15: 702–703
Fischler B, Rodensjo P, Nemeth A, Forsgren M, Lewensohn-Fuchs I (1999) Cytomegalovirus DNA detection on Guthrie cards in patients with neonatal cholestasis. Arch Dis Child Fetal Neonatal Ed 80: F130–F134
Gale KB, Ford AM, Repp R, Borkhardt A, Keller C, Eden OB, Greaves MF (1997) Backtracking leukemia to birth: identification of clonotypic gene fusion sequences in neonatal blood spots. Proc Natl Acad Sci USA 94: 13950–13954
Gilman EA, McNally RJ, Cartwright RA (1999) Space–time clustering of acute lymphoblastic leukaemia in parts of the U.K. (1984–1993). Eur J Cancer 35: 91–96
Greaves M (1999) Molecular genetics, natural history and the demise of childhood leukaemia. Eur J Cancer 35: 1941–1953
Gustafsson A, Levitsky V, Zou JZ, Frisan T, Dalianis T, Ljungman P, Ringden O, Winiarski J, Ernberg I, Masucci MG (2000) Epstein–Barr virus (EBV) load in bone marrow transplant recipients at risk to develop posttransplant lymphoproliferative disease: prophylactic infusion of EBV-specific cytotoxic T cells. Blood 95: 807–814
Gustafsson B, Carstensen J (1999) Evidence of space–time clustering of childhood acute lymphoblastic leukaemia in Sweden. Br J Cancer 79: 655–657
Gustafsson B, Carstensen J (2000) Space–time clustering of childhood lymphatic leukaemias and non-Hodgkin's lymphomas in Sweden. Eur J Epidemiol 16: 1111–1116
Hall CB, Long CE, Schnabel KC, Caserta MT, McIntyre KM, Costanzo MA, Knott A, Dewhurst S, Insel RA, Epstein LG (1994) Human herpesvirus-6 infection in children. A prospective study of complications and reactivation. N Engl J Med 331: 432–438
Isa A, Priftakis P, Broliden K, Gustafsson B (2004) Human parvovirus B19 DNA is not detected in Guthrie cards from children who have developed acute lymphoblastic leukemia. Pediatr Blood Cancer 42: 357–360
Kinlen L, Jiang J, Hemminki K (2002) A case–control study of childhood leukaemia and paternal occupational contact level in rural Sweden. Br J Cancer 86: 732–737
Kinlen LJ, Balkwill A (2001) Infective cause of childhood leukaemia and wartime population mixing in Orkney and Shetland. Lancet 358: 155
Kinlen LJ, Clarke K, Hudson C (1990) Evidence from population mixing in British New Towns 1946–85 of an infective basis for childhood leukaemia. Lancet 336: 577–582
Knox EG, Stewart A, Kneale G (1980) Childhood leukaemia and mother–foetus infection. Br J Cancer 42: 158–161
Lehtinen M, Koskela P, Ogmundsdottir HM, Bloigu A, Dillner J, Gudnadottir M, Hakulinen T, Kjartansdottir A, Kvarnung M, Pukkala E, Tulinius H, Lehtinen T (2003) Maternal herpesvirus infections and risk of acute lymphoblastic leukemia in the offspring. Am J Epidemiol 158: 207–213
Matsuda Y, Hara J, Miyoshi H, Osugi Y, Fujisaki H, Takai K, Ohta H, Tanaka-Taya K, Yamanishi K, Okada S (1999) Thrombotic microangiopathy associated with reactivation of human herpesvirus-6 following high-dose chemotherapy with autologous bone marrow transplantation in young children. Bone Marrow Transplant 24: 919–923
Ohls R, Christensen R. (2000) The development of the hematopioetic system. In Nelson Textbook of Pediatrics, Behrman R, Jenson H (eds) pp 1456. Philadelphia: Saunders Company
Peckham CS (1991) Cytomegalovirus infection: congenital and neonatal disease. Scand J Infect Dis Suppl 80: 82–87
Petridou E, Revinthi K, Alexander FE, Haidas S, Koliouskas D, Kosmidis H, Piperopoulou F, Tzortzatou F, Trichopoulos D (1996) Space–time clustering of childhood leukaemia in Greece: evidence supporting a viral aetiology. Br J Cancer 73: 1278–1283
Priftakis P, Dalianis T, Carstensen J, Samuelsson U, Lewensohn-Fuchs I, Bogdanovic G, Winiarski J, Gustafsson B (2003) Human polyomavirus DNA is not detected in Guthrie cards (dried blood spots) from children who developed acute lymphoblastic leukemia. Med Pediatr Oncol 40: 219–223
Rickinson AB, Kieff E (1996) Epstein–Barr virus. In Fields Virology, Fields BN, Knipe DM, Howley PM (eds) 3rd edn, pp 2397–2446. Philadelphia, PA: Lippincott-Raven
Ross JA (1999) Epidemiologic studies of childhood leukemia: where do we go from here? Med Pediatr Oncol 32: 65–67
Saiki RK, Bugawan TL, Horn GT, Mullis KB, Erlich HA (1986) Analysis of enzymatically amplified beta-globin and HLA-DQ alpha DNA with allele-specific oligonucleotide probes. Nature 324: 163–166
Salahuddin SZ, Ablashi DV, Markham PD, Josephs SF, Sturzenegger S, Kaplan M, Halligan G, Biberfeld P, Wong-Staal F, Kramarsky B, Gallo RC (1986) Isolation of a new virus, HBLV, in patients with lymphoproliferative disorders. Science 234: 596–601
Salonen MJ, Siimes MA, Salonen EM, Vaheri A, Koskiniemi M (2002) Antibody status to HHV-6 in children with leukaemia. Leukemia 16: 716–719
Smith M (1997) Considerations on a possible viral etiology for B-precursor acute lymphoblastic leukemia of childhood. J Immunother 20: 89–100
Tolfvenstam T, Papadogiannakis N, Norbeck O, Petersson K, Broliden K (2001) Frequency of human parvovirus B19 infection in intrauterine fetal death. Lancet 357: 1494–1497
Wang FZ, Dahl H, Linde A, Brytting M, Ehrnst A, Ljungman P (1996) Lymphotropic herpesviruses in allogeneic bone marrow transplantation. Blood 88: 3615–3620
Wiemels JL, Cazzaniga G, Daniotti M, Eden OB, Addison GM, Masera G, Saha V, Biondi A, Greaves MF (1999) Prenatal origin of acute lymphoblastic leukaemia in children. Lancet 354: 1499–1503
Acknowledgements
We would like to thank Britta Lindqvist and Marie Sandberg for their excellent work in organising the neonatal spots; Claes Gutenberg Associate Professor, head of the PKU-Laboratory, for providing us with Guthrie cards; Helena Dahl for providing us with sera from a patient who developed a HHV-6 infection. This study was supported by grants from the Mary Béves Foundation, the Tobias Foundation, the Swedish Child Cancer Foundation, the Swedish Cancer Foundation, the Stockholm Cancer Society, and the Stockholm City Council and the Karolinska Institutet.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Bogdanovic, G., Jernberg, Å., Priftakis, P. et al. Human herpes virus 6 or Epstein–Barr virus were not detected in Guthrie cards from children who later developed leukaemia. Br J Cancer 91, 913–915 (2004). https://doi.org/10.1038/sj.bjc.6602099
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6602099
Keywords
This article is cited by
-
Cytomegalovirus infection may be oncoprotective against neoplasms of B-lymphocyte lineage: single-institution experience and survey of global evidence
Virology Journal (2022)
-
DNA damage signalling from the placenta to foetal blood as a potential mechanism for childhood leukaemia initiation
Scientific Reports (2019)
-
Virome characterisation from Guthrie cards in children who later developed acute lymphoblastic leukaemia
British Journal of Cancer (2016)
-
Seroprevalence of Human Herpes Simplex, Hepatitis B and Epstein-Barr Viruses in Children with Acute Lymphoblastic Leukemia in Southern Iran
Pathology & Oncology Research (2010)
-
Adenovirus detection in Guthrie cards from paediatric leukaemia cases and controls
British Journal of Cancer (2008)
