
Abstract
Data sources
Electronic searches of PubMed, the Cochrane Library, Embase, the National Health Service Economic Evaluation Database and HTA until March 2017. Also handsearched referenced in the original articles. Grey literature was not included.
Study selection
Randomised controlled trials with more than ten participants with oro-facial pain duration of more than three months were sub grouped into: TMD-muscle pain (TMD-m), TMD-joint pain (TMD-j), burning mouth syndrome (BMS) and other oro-facial pain. Studies include any pharmacological treatment against another pharmacological, non-pharmacological treatment, placebo or no treatment. The primary outcome was change in pain intensity and the secondary outcome was the effect on quality of life.
Data extraction and synthesis
Three authors formed three review pairs that independently checked for inclusion. Four pairs of reviewers independently evaluated the risk of bias using the Swedish Agency for Health Technology Assessment and Assessment of Social Services tool. Two authors independently extracted data that were later assessed according to a modified GRADE system.
Results
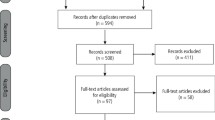
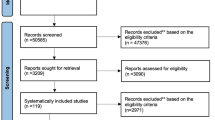
Forty-one studies, rated medium to low risk of bias, were included in qualitative analysis on patients with TMD-j pain (15 studies, n = 790), TMD-m pain (nine studies, n = 375), BMS (17 studies n = 868). For the TMD-j group five studies support NSAIDs and nine corticosteroid and hyaluronate injections. Eight of the nine TMD-m studies were included in a network meta-analysis (NMA), they support cyclobenzaprine, botulinum toxin injections and topical treatment with Ping-On ointment. Five of the 17 BMS studies included in a NMA support topical capsaicin and clonazepam. Of the remaining 12, five showed no effect while the remaining support alpha lipoic acid, gabapentin, clonazepam, amisulpride and SSRIs.
Conclusions
Based on the results of the NMA the authors concluded that clonazepam and capsaicin are effective for BMS while cyclobenzaprine, a muscle relaxant, has a positive treatment effect on TMJ-m. Evidence from the narrative synthesis suggests NSAIDs, corticosteroid and hyaluronate injections are effective for TMD-j pain.
Similar content being viewed by others

Commentary
This is a systematic review that attempts to evaluate the efficacy of various pharmacologic treatments for three different categories of oro-facial pain: temporomandibular muscle disorders (TMD-muscle), temporomandibular joint disorders (TMD-J) and burning mouth syndrome (BMS). The first two may have some overlap of diagnoses. The prevalence of TMD-arthritis and TMD-disc displacement is relatively low compared to TMD-muscle pain; however, these two joint sub-groups are commonly diagnosed in conjunction with TMD-muscle pain.1
BMS is an unrelated neuropathic disorder diagnosed with symptoms of oral mucosal burning and the exclusion of oral mucosal disease. BMS is most common in post-menopausal women, with prevalence rates in the general population varying between 0.1%-3.9%2 with a recent population-based study showing a prevalence of 0.11%.3
It is not clear in the review which diagnostic criteria were accepted for inclusion in any of the categories. There are research standards, the most recent being the Research Diagnostic Criteria (RDC) for Temporomandibular Disorders for the diagnosis and categorisation (muscle, disc displacement or arthritis) of temporomandibular disorders.4 Without standard diagnostic criteria, the nature and the severity of the conditions included are uncertain.
It should also be noted that patients with rheumatic disorders were excluded from this study, which could greatly affect the results on TMD-joint, as arthritis is one sub-category of this disorder. As for BMS, since the diagnosis is made by exclusion it is important to know which conditions were indeed excluded.
The studies included topical, local and systemic pharmacologic interventions, with varying doses and durations. Since the results were based on the combined effect of an individual agent, it is uncertain which aspect is responsible for the observed effects such as the agent, the delivery, the duration or the dose.
It was beneficial that this review only used visual analog scales (VAS) for outcome measures of pain reduction. Only five of the forty-one studies measured quality of life and found no effect on quality of life.
The use of the NMA offers the advantage of allowing comparison of multiple interventions in a single review. For the TMD-joint group, the included studies were not eligible for NMA, however the authors suggested there is evidence supporting the use of NSAIDs, and corticosteroid and hyaluronate injections. For the TMD-muscle group the NMA (eight studies) supports evidence of the pain-reducing effect of cyclobenzaprine (a muscle relaxant); however, there was only a three-week follow-up. For BMS, five studies were included in the NMA, and based on the authors' interpretation, it supports the pain-reducing effects of clonazepam (a benzodiazepine commonly used for neuropathic pain) and topical use of capsaicin (a substance found in chilli peppers that causes nerve desensitisation thereby reducing pain signals). Of the three clonazepam studies, two were topical and one was systemic, with varying frequencies and durations from two weeks to two months duration. Only one capsaicin study was included in the NMA, which also compared the use of alpha lipoic acid and lactoperoxidase, all of which showed statistically significant effect in pain reduction but no significant difference between groups. It is unclear how the superiority of capsaicin was established. In this review, with so few eligible studies, NMA may not be able to offer an advantage.
By far, the data in this review are insufficient to determine which pharmacologic interventions provide the best pain relief in any of these oro-facial pain conditions.
The range of duration of the individual studies (two weeks up to six months) may be too short to understand the effect on a chronic condition that may require long-term treatment. When studying therapeutic effects on a chronic pain condition, long-term follow-ups are needed.
Also evidence is lacking for short and long-term side effects, quality of life and cost.
References
Lobbezoo F, Drangsholt M, Peck C, Sato H, Kopp S, Svensson P . Topical review: new insights into the pathology and diagnosis of disorders of the temporomandibular joint. J Orofac Pain 2004; 18:181–191.
McMillan R, Forssell H, Buchanan JA, Glenny AM, Weldon JC, Zakrzewska JM . Interventions for treating burning mouth syndrome. Cochrane Database Syst Rev 2016; 11:CD002779.
Kohorst JJ, Bruce AJ, Torgerson RR, Schenck LA, Davis MD . The prevalence of burning mouth syndrome in a population-based study. Br J Dermatol 2015; 172:1654–1656.
Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest group. J Oral Facial Pain Headache 2014; 28:6–27.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Birgitta Häggman-Henrikson, Department of Orofacial Pain and Jaw Function, Faculty of Odontology, Malmö University, Malmö, Sweden. E-mail: birgitta.haggman.henrikson@mah.se
Häggman-Henrikson B, Alstergren P, Davidson T, Högestätt ED, Östlund P, Tranaeus S, Vitols S, List T. Pharmacological treatment of oro-facial pain - health technology assessment including a systematic review with network meta-analysis. J Oral Rehabil2017; 44: 800-826. doi: 10.1111/joor.12539. [Epub ahead of print] Review. PubMed PMID: 28653747.
Rights and permissions
About this article

Cite this article
Fischoff, D., Spivakovsky, S. Are pharmacological treatments for oro-facial pain effective?. Evid Based Dent 19, 28–29 (2018). https://doi.org/10.1038/sj.ebd.6401294
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401294
