
Key Points
-
Demonstrates that over 90% of oral healthcare in Romania is funded privately – some public support is available for children.
-
Suggests there has been an overproduction of dentists for several years and low uptake of dental services.
-
Notes that on 31 December 2014, out of 14,841 Romanian qualified dentists 616 were registered with the General Dental Council in the United Kingdom.
Abstract
Romania is one of the newest member states of the European Union (EU). It has 13 dental schools, 14,841 dentists and 2,935 dental technicians providing oral health care for a population, at 31 December 2014, of 21.3 million. The shift from a communist system to a democratic or capitalist society has contributed to an enormous change in the proportion of public and private sector oral health services. The lack of public funds during the post-communist years has contributed to a dependency on private oral healthcare rather than the government financed public provision. Affordability and social awareness have together established a mixed economy for oral health care costs and oral healthcare is growing slowly compared with other developed EU member states. At the same time, there has been overproduction of new dentists (currently 1500 graduate annually). This has led to un and under-employment and emigration of dentists to other EU member states. This paper explains the current oral healthcare system in Romania and changes in recent years.
Similar content being viewed by others

Introduction
Romania is located in the South East of Europe, in the North of the Balkan Peninsula. In 2014, it had a population of just over 21 million, several of whom are currently living in other EU member states. The density of the population is around 84 inhabitants/km2. The number of towns is 320 and the number of villages 2861, with an additional 12,957 small villages. Approximately 12 million people (54%) live in urban areas and about 10 million (46%) in rural areas.1
In the last 20 years, Romania has made considerable progress in developing institutions compatible with a market economy. Joining the European Union (EU) in 2007 was a driving force for reform and modernisation. Challenges to accelerate growth in the country include uncertainty in the Euro zone and export markets, political developments and availability of EU funds. The key challenges for Romania have been and are to achieve steady economic growth and improve living standards while meeting fiscal targets, and to continue structural reforms and the modernisation of public administration, health and education.
This paper will cover the following aspects:
-
The insurance-based healthcare provision system
-
Reimbursement of costs of oral healthcare
-
Oral health services
-
Prevention and oral health promotion
-
Oral healthcare workforce
-
Oral health and use of dental services
-
Dental education
-
Specialist training
-
Epidemiology
-
Costs of health and oral health.
Aim
The aim of this paper is to describe the provision of the oral healthcare system in Romania. The pre and immediately post communist era and post EU membership years, and economic and social influence will be discussed.
Insurance-based healthcare provision system
The provision of health services is the responsibility of the Romanian Government through the Ministry of Public Health. The current health insurance system was founded in 1998 and it is administered centrally by the National Health Insurance House (NHIH), which is divided into 42 district houses of health insurance, corresponding to the 41 Romanian counties and the city of Bucharest.
The health insurance system insures the whole population. The system also incorporates health insurance specially designed for certain categories of patients, who have their own health insurance houses. There is the Health Insurance House for Defence, Public Order, National Security and Judicial Authority (OPSNAJ). It covers the needs of the military personnel, police and people in the judicial system. Workers in transport, communications and tourism are insured with the Health Insurance House for The Ministry of Transport, Constructions and Tourism (CASMTCT).
The health insurance system is based on the Bismarkian model. In 2015, all workers contribute the equivalent of 10.7% of their total pay, of which the insured person pays 5.5% and their employer 5.2%.
According to article 213 §1 of the Law 95/2006, certain categories of people are covered by health insurance but are exempt from paying the contributions. They are:
-
All children and young people up to 26 years in school, high school graduates, apprentices and students who receive no income from work; young people on guaranteed minimum income
-
Husbands, wives and parents with no personal income who are dependents of an insured person
-
Some other groups such as war veterans and those who were persecuted, before 1990 under the communist dictator
-
People with disabilities or some illnesses, with no income
-
Pregnant and puerperal women, if they have no income or have incomes below the national minimum gross wage.2
As in the United Kingdom, medical care is paid for from a mixture of private and public funds. Primary medical care is provided by doctors who own their own practices (offices) and have contracts with the state insurance system, with private insurers and with individual patients. Hospitals are also funded both publically and privately.
In contrast to the situation before 1990, when nearly all dentists were salaried employees of the State, only a minority are now salaried. They work in universities and the defence forces. All other dentists can be described as private. In 1990, shortly after the communist era ended, private dental practices were rapidly established. There were and are two types.3 One is the individual dental practice (office), comprised of just one dentist and/or associates working as a team. The other type is large scale limited liability companies for dental treatment services, comprising more than two dental practices (offices) with large workforces. In 2012 there were 12, 904 individual dental offices (the first type) and 197 owned by dental medical companies (the second type).
There is at least one emergency dental clinic in each of the 41 Romanian counties. Some of these are situated in hospitals, others in close proximity to dental schools and others are part of larger medical centres.
Reimbursement of costs of oral healthcare
Oral healthcare has been funded by the public health insurance system since 1998. However, reimbursement of oral healthcare by the statutory Health Insurance System is limited. Children and young people under 18 years of age are theoretically covered for: an annual examination; preventive treatment (oral hygiene, fissure sealants); dental radiography (including intra- and extra-oral views); conservative treatment (including composite fillings); endodontic treatment; periodontal treatment; prosthetic treatment (acrylic dentures, resin crowns, resin with metal crowns); orthodontic treatment (removable and functional orthodontic appliances, space retainers; advice on controlling habits such as thumb sucking); oral surgery (extractions, alveolar surgery; emergency immobilisation of the maxillary fractures); and examination for oro-medical problems (cancer, ulcers, and so on).
The statutory insurance scheme also pays 60% of the costs of dental treatment of adults' extractions, acrylic complete and partial dentures and resin with metal crowns. Overall, it has been estimated that patients pay 90% of the cost of their dental treatment themselves, while costs of some prosthetic treatments (ceramic crowns, metal-based dentures, prostheses covering implants), fixed orthodontic appliances, periodontal surgery and dental implants are not covered at all. The patients, or invariably their parents, have to pay the dentist for these treatments.4
Only a minority of dental practices have contracts with the National Health Insurance House (NHIH), leading to major access problems for patients. The total fee paid to each dentist, for the services provided to all children, varies slightly from country to county. Currently, a fixed fee of around €300 (£210) per month is paid to general dentists and €400 (£280) per month to dental specialists. These are gross and not net fees and are low even by Romanian standards. Therefore, it is perhaps unsurprising that in 2015, only 2,613 dental practices (offices) out of a total of just under 13,000 are currently in contract with and reimbursed by the (NHIH).
Thus, the funds allocated by the NHIH rarely cover the costs of all the treatment a dentist provides to those under 18 years of age.
Prevention and oral health promotion
At a local level there have been some prevention and oral health promotion schemes in some parts of Romania. For example, a fluoride mouth rinsing programme in schools in Constanta and Iasi counties was initiated in 2000 and ran until 2007. This programme was funded by the Ministry of Public Health in order to reduce the prevalence of caries in school children in grades 1-4 (6–11 years old). The programme provided oral health education and also introduced supervised fluoride mouth rinsing, with a neutral fluoride solution containing 0.275% sodium fluoride (Fluorostom, produced by the National Institute of Chemical–Pharmaceutical Research, ICCF,Bucharest), every week in grades 1-4 in both counties.5
Oral healthcare workforce
According to data provided by the National Public Health Institute-National Centre for Statistics and Informatics in Public Health (INSP-CNSISP), in 2013, Romania had 14,282 dentists with a density of 6.7 dentists per 10,000 inhabitants (Table 1).6 Out of all dentists, 2,809 were registered in the public sector and were providing services for the NHIH. The distribution of dentists by counties in Romania shows the largest numbers are in Bucharest (3,349), followed by Cluj (972), Timis (938), Iasi (849) and Constanta (667) counties, all of which include major cities with dental schools (Table 2).7
On graduation, all dentists are registered by the College (Board) of Dentists. In July 2015, the number of registered dentists was 14,841.7 Professional monitoring of the dentists (dentists' data, qualifications and dealing with complaints from patients) is carried out at a district level.
Looking retrospectively, according to the College of Dentists in Romania (CMDR) there were 16,486 dentists in 2010. According to the Handbook of Dental Practice published by the European Council of Dentists in 2008: 68% were women and 32% men, the total number of dental hygienists was 100, total number of dental nurses: 6,000, total number of dental technicians: 6,000 and the total number of specialists in: oral surgery: 157, orthodontics: 412, maxillofacial surgery: 234.8
The number of people working in dental laboratories increased from 3,200 in 2002 to 6,980 in 2007. Most of them work in private laboratories. Since 2007, dental technicians have been required to register with the Order of Romanian Dental Technicians. At December 31, 2014, there were 2,935 registered dental technicians.9 Their distribution across the country is shown in Table 2.
Dental hygienists and nurses must be registered with the Order of Nurses, Midwives and Medical Assistants.10 The percentage of dentists that are employing dental nurses (chair-side assistants) to help them is under 20%. There are currently approximately 5,900 dental nurses assisting dentists in Romania. Because of migration to other countries and the rapid expansion in the numbers of dentists, at present Romania faces a critical shortage of dental nurses. Unfortunately, at present, the numbers entering schools of dental nursing are very low because dental nurses (chair-side assistants) are very poorly paid.
Oral health and the use of dental services
According to a study of oral healthcare in Romania conducted by IPSOS Research in 2012: from a sample of 500 people, men and women aged between 18 and 65 years, in urban areas (representative national sample for urban areas), 80% of Romanians were found to have dental problems, tooth decay being the most common disorder (71%). Four out of ten people had poor plaque control, while three out of ten had halitosis and sensitive teeth.11
Although 80% of Romanians may have dental problems, it was also found in this study that they show a strong reluctance to go to the dentist – 49% have not visited a dental office in the past year, while only 29% went to the dental office for a check-up. In addition, 9% of Romanians claim to have never been to the dentist. The main reason mentioned by 64% of the participants in the study was the high cost of dental treatments.11
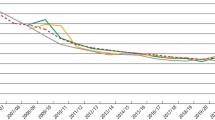
The number of all dental examinations including those funded by the NHIH and those paid for privately was 716,800 in 2013, compared with 7,718,900 in 2007 (Table 3). This dramatic fall reflects the economic crisis, probable underreporting of privately funded dental examinations and the low fees offered by the NHIH.
In parallel with the fall in the number of examinations funded by the NHIH, there was a decreasing trend in the number of dental examinations and treatments in Romania, from 0.07 examinations and treatments per inhabitant in the year 2011 to 0.03 in 2012 and 2013, probably due to deficiencies in reporting by dental offices. Expenses allocated to oral healthcare services are closely correlated with GDP. According to the 2012 report of the 'European Platform for Better Oral Health', Romania has the lowest per capita expenditure on oral health in the European Union.12 However, this was an estimate and may only have included treatment funded by the NHIH and not privately.
Dental education
Dentists train in one of the 13 dental faculties of Romanian universities, of which nine are public (state) faculties and four are private. All those who attend private dental schools pay fees.
Since 2004, the Government has paid the fees of students who have attended state dental schools and gained the highest marks in their school leaving examinations. The remaining 30–50% of students, who have lower marks, pay their own fees (between £1,000 and £1,600 per year). Currently, 1,500 new Romanian dentists graduate each year. In addition, some dental schools run courses for non-Romanian students in English and French. This overproduction has existed for some years and few new dental graduates can find full-time work in Romania. As a result, many choose to work in other EU Member States such as Germany, Italy and the United Kingdom, where 616 were registered with the General Dental Council on 31 December 2014.
Since 1990, dental education has lasted for six years. Basic sciences are studied in the first 18 months, general medicine in the next 18 months, and clinical dentistry in the final three years. After graduating from university and passing licensing examinations, newly qualified dentists obtain a licence to practice (practicing certificate), which entitles them to practice independently as general dental practitioners.
One of the most important duties of dentists, as a necessary condition for continuing dental practice, is to undertake continuing professional education (CPE) in order to maintain their registration. A range of activities (such as courses, seminars, conferences) are organised by dental associations and dental faculties (schools). The activities are delivered by the staff of the dental faculties (schools) and other dentists with experience and professional probity, accredited by the Romanian Council of the College (Board) of Dentists. All dentists must complete a minimum of 200 credit points (one hour's CPD equals 1 credit point) of CPE every five years and register these hours in a special registry held at county level. At the end of each 5-year period, dentists must prove they have achieved the minimum number of credit points. In case of non-compliance with these requirements, dentists are liable to financial sanctions and/may have their practicing licence suspended.
Education of dental hygienists started in five public universities in 1975, but was stopped after a few years. In 1995, the system started again and a few more dental hygienists graduated. In 2002, the law was changed and training stopped again. However, in 2007, after pressure from the Romanian Association (Platform) of Oral-Dental Public Health, dental hygienist training was resumed. The training course takes place at the faculty of dental medicine in Timisoara and lasts for three years. Students pass a qualifying examination and get a licence to practice. Dentists must prescribe the treatment that dental hygienists provide and they have to work in a dentist's practice (office).
After a final examination, those who are successful are awarded a diploma and must be registered with the Order of Nurses, Midwives and Medical Assistants in Romania. They are required to complete CPE throughout their careers in order retain the right to practice. Currently, dental hygienists are trained only in Timisoara.
Dental technicians are trained in dental technician colleges organised by the dental medicine faculties. Training lasts for three years and ends with a qualifying examination. Those who pass are awarded a diploma and must register with the Order of Romanian Dental Technicians. Technicians are required to complete CPE throughout their careers in order retain the right to practice.
Specialist training
Currently, six dental specialties are recognised in Romania and about 300 enter specialist training annually. The specialties are oral maxillofacial surgery, oral surgery, orthodontics, periodontics, prosthodontics and endodontics. At present, annually, universities establish a fixed number of training places for each speciality. The number of training places varies from year to year. Admission to specialist training is subject to an examination organised in one of the six centres that train specialists (Bucharest, Timisoara, Iasi, Targu Mures, Cluj, Craiova). Dentists who wish to specialise compete for training appointments.
Postgraduate studies leading to a Masters degree have been established by the universities. The programmes cover the following topics: implantology and prosthodontics (at Targu Mures), Implant prosthetic rehabilitation of edentulous, oral rehabilitation and aesthetics, techniques in aesthetics and restoration, lasers in dentistry (at Iasi), Non-invasive methods of diagnosis and laser treatment in dentistry and law in dentistry (at Timisoara), and Forensic dentistry (at Cluj Napoca).13-15
Apart from oral-maxillo facial surgery, training in the other five specialties is full-time and lasts for three years. For maxillofacial surgery, there is a five-year training period and it also requires graduation in general medicine. The training programmes take place in accredited universities and follow curricula set out in the European Commission's Training Directives. When training, the dentists are paid a salary by the Ministry of Public Health but are forbidden to work in private practice during their training years. At the end of training, they receive a specialist degree and diploma recognised by the Ministry of Public Health.16 Many would like more specialties to be recognised in Romania, as they are in Poland, Sweden, and the United Kingdom. However, movement to create additional specialties has so far been unsuccessful because they have been thwarted by one of Romania's dental associations.
Epidemiology
In 1992, a national survey was performed using the WHO Pathfinder protocol. It suggested that the national mean DMFT for 12-years-olds was 4.1.17 A follow up survey, which also used the WHO Pathfinder protocol, was performed in 2000. It suggested that in that year the national mean DMFT for 12-year-olds was 2.8.18
A number of local surveys of children have taken place. In 2011 a survey of the caries prevalence of 6-8 and 11-13-year-old children was performed in Bucharest, Iasi, Cluj Napoca, Timisoara and Targu Mures.19 Mean dmft for 6-8-year-olds ranged from 3.3 in Bucharest to 5.3 in Cluj Napoca.
Mean DMFT for 11-13-year-olds ranged from 1.5 in Bucharest to 5.6 in Timisoara.19 There have been no national oral epidemiological surveys of adults.
Lip and oral cavity cancer in Romania is an important public health problem, with high incidence and mortality. Data provided by the International Agency for Research on Cancer suggests that Romania ranks ninth in Europe in terms of number of new cases of cancers of the mouth and lips and is in sixth place if incidence and mortality rates created by these conditions are taken into account.20 In 2010, according to EU statistics, 29% of men and 30% of women in Romania were smokers. In 2014 the percentage of smokers declared at EU level was 26% men and 27% women.21 Total, annual alcohol per capita consumption (APC) in the population over the age of 16 years in 2010 was 14.4 litres.21
Cost of health and oral health
Romania ranks last in the European Union in terms of health expenditure as percentage of GDP, according to Eurostat data in 2012. Public (state) expenditure on health in Romania was around 4% of GDP. In comparison, in France, Germany, the Netherlands and Denmark, over 11% of GDP was allocated to health. In Central and Eastern Europe, Poland spent 7% of GDP on health, Hungary spent 8% and the Czech Republic spent 7.5%. Overall, the EU average percentage of GDP allocated to health was around 10% in 2012.22
Regarding the amount spent for each citizen in the EU, in Romania approximately €720 (£516) per citizen was spent in 2012, while Poland was spending about €1,350 (£930), Hungary spent €1,750 (£1200), Czech Republic and Spain both spent €2,835 (£2,025) and the EU average health expenditure per citizen was approximately €3,015 (£2,150).23
As for oral health, public funding of €14 million (57.9 million RON – £10 million) in 2012 (that is, 0.2% of the Health budget) was distributed among the 2,800 dentists who were in contract with the Health Insurance House. It dropped to €3 million (13 million RON – £2.15 million) in the first quarter of 2013, when approximately 1,780 dentists remained in contract with NHIH. No budget was allocated from April 2013 to June 2014, when the funding of dental services was resumed (Table 4). As mentioned earlier, rules for the framework contract for healthcare delivery in 2013-14 theoretically provide basic healthcare service packages for prevention and dental treatments to be delivered and totally reimbursed by the NHIH for children aged up to 18 years of age and for beneficiaries of the special laws detailed earlier in this paper. Among the services that should be reimbursed by NHIH are: examinations; simple caries treatment; treatment of dental pulp disorders; extractions; acrylic dentures fitting; and revision. In March 2013 the budget fell to 30%, and then in April 2013 to zero. Thus, in the last four years, there has been very little public funding for oral healthcare and most patients have had to pay for their oral healthcare themselves.
Discussion
As has been described, the oral healthcare system in Romania is dominated by the private sector. Many of the data presented in this paper on costs, attendances for dental visits and other topics are unlikely to be as accurate as those from other EU member states as they relate to the private sector, are often estimates and are not collected either locally or centrally. There are 11,460 private dental practices (offices) registered with the government as oral healthcare businesses and they comprise almost 90% of all dental practices in Romania. The other 10% is made up by university dental outpatient units serving local people for emergency dental treatments, defence services dental clinics etc, and are publically funded. The number of patients treated annually in the public and private sectors is far from clear as there are no local or national electronic patient databases, nor a system for collating paper records. However, recently, the Ministry of Public Health has introduced a health-card system, which will synchronise the oral healthcare data provided within the NHIH, but not under private arrangements and record all dental treatment provided within the public sector.
A previous description of the system for the provision of oral healthcare in Romania, referred to data for 2007 from the Ministry of Public Health and stated that the proportion of expenditure budget for preventive programme was as low as 0.6% of the total public sector budget for oral healthcare.24 In view of the prevalence of dental caries, periodontal diseases and oral cancer, this is a woefully small sum.
During the Communist period (1947-1989), the healthcare system was run by the government and all dental professionals were under the umbrella of the government's scheme and policy. Oral healthcare was given a lower priority than general healthcare. The four decades were dominated by the governmental monopoly over health services and primary care was provided at dispensaries for primary healthcare under the Semashko system.25 This led to a significant improvement in public health provision and there was universal and equal access to healthcare for all the citizens. Life expectancy increased from 65 years in 1956 to 77.5 years in 2011 (for women) and from 61.5 years in 1956 to 70.1 years in 2011 (for men).26 Reforms were introduced in 1983 and included the free choice of your own doctor and dentist. However, in the last years of the Communist period (1985-1989) the system became unproductive as the unmet needs for more funding increasingly limited any further improvements.
The private sector provides all types of dental treatment from emergency treatments to aesthetic (cosmetic) dentistry. In common with those in other EU member states, the Romanian middle and higher income groups now increasingly understand the importance of good oral health and wish to have 'a nice smile'. In the last ten years, over two million Romanians have gone to work in other EU member states. Influences from other EU member states' cultures have helped the development of competitiveness in costs and improvisation within dentistry in the private sector. The Romanian citizens, who have migrated to work elsewhere in the EU, send money back to their home country and make substantial contributions to the national economy. In general, they choose to receive dental treatment in Romania rather than in the member state that they have migrated to as in Romania they can receive a high quality of dental treatment at the lowest costs in Europe.
Most of the private sector dental offices are equipped with new and modern dental equipment. Romanian universities are increasingly involved in joint research programmes and initiatives with other EU member states. These factors have led to the embryonic development of dental tourism, with patients from economically more developed countries coming to Romania for dental treatment, where the cost of the dental treatment is approximately a quarter of the same treatment in the UK, Germany, France or Italy. As has previously been mentioned, very little government (public) money is spent on the prevention of oral disease. It is therefore heartening that at a local level private dental practices have started to work with dental product manufacturers to raise awareness in the local communities of the need for good oral health. One such programme, supported by an oral care company, is the 'Smile Romania' campaign, which started in 2012. It focuses on educational programmes related to oral hygiene. It provides free oral hygiene products and educational courses which emphasise the importance of oral health. In 2015 the campaign is ongoing.27
Although some public funds are allocated to the oral healthcare of children and young people, the oral healthcare for disabled (special needs) children and adults is poor. They are neither supported properly by the government nor by the dental professionals due to lack of knowledge of how to treat them and a general neglect of the disabled community. There is a particular problem for special needs patients and others living in rural areas. This is because many people in rural areas do not have cars and public transport is often non-existent. Furthermore, apart from a very small number of public clinics, the dental practices are generally located in towns and cities. Unfortunately, there has been no effort by the Ministry of Public Health to address these problems due to the lack of research in community oral healthcare and its synchronisation with the national healthcare system.
In view of all these challenges it is unsurprising that the uptake of oral healthcare in Romania is low. It was estimated that in 2009, only 34% of Romanians visited a dentist.28 The reduction in government spending and the economic crisis may have subsequently further reduced this percentage as well as the fact that between April 2013 and June 2014 funding from the National Health Insurance House was stopped.
Conclusion
The provision of oral healthcare in Romania faces numerous challenges. They have arisen because of the rapid change from a communist system, which attempted to provide universal healthcare for all, but was highly inefficient and bureaucratic, to a capitalist free market economy in which there has been little planning and governmental involvement in public health. If improvements are to be made it will be necessary for all those involved (the dental profession, government and patients) to work together.
References
Widström E, Eaton K A . Systems for the Provision of Oral Health Care, Workforce and Costs in the European Union, European Economic Area and Accession States in 2003 – A Council of European Chief Dental Officers Survey. Oral Health Prev Dent 2004; 2: 155–194.
Ministry of Public Health. Monitoring the inequalities in health condition of Romanian population in the year 2013. National Public Health Institute. Available online at http://insp.gov.ro/sites/cnepss/wp-content/uploads/2014/11/INEGALITATI-2014.pdf (accessed July 2015).
National Institute of Statistics. The activity of hospitals (sanitary units) Available online at http://www.insse.ro/cms/files/publicatii/Activitatea%20unitatilor%20sanitare%202012.pdf (accessed August 2015).
College (Board) of Dentists in Romania. Basic health services for dentistry. Available online at http://www.cmdr.ro/images/products/Anexele+nr+14-16+Normelo_35684.pdf (accessed August 2015).
Danila I, Amariei C, Nuca C, Bobu. L . The Romanian National Programme for Caries Prevention: The Experience of Iasi and Constanta Centres, Romania, 2000–2007. Oral Health Dent Manag Black Sea Count, 2010; 9: 88–97.
National Public Health Institute.National Centre for Statistics and Informatics in Public Health (INSP-CNSISP). Health Care Statistical Yearbook 2014. Available online at http://dspbn.bistrita.ro/wp-content/uploads/ASsano.pdf (accessed July 2015).
College (Board) of Dentists in Romania. Dentists Register. Available online at http://www.cmdr.ro (accessed July 2015).
National Institute of Statistics. The analysis of situation in Romania with the occasion of World Oral Health Day, 20th March, 2014. Available online at http://www.dspiasi.ro/images/analiza_situatie_sanatateorala_201403_pdf (accessed July 215).
Order of Romanian Dental Technicians. Technicians Register 2014. Available online at http://www.otdr.ro/files/rutd.pdf (accessed July 2015).
Order of Nurses, Midwives and Medical Assistants in Romania. [Homepage]. Available online at http://www.oamr.ro (accessed July 2015)
Study I P S OS Research. Oral Care, utilization and attitudes; May 2012; in Romania-applied on a sample of 500 people, men and women 18–65 years old, urban (national representation in urban area). Available online at http://www.dspalba.ro/promovare/oral2015/analiza.pdf (accessed July 2015).
Patel R . The State of Oral Health in Europe- A report for the Platform for Better Oral Health in Europe 2012. Available online at www.oralhealthplatform.eu/our-work/the-state-of-oral-health-in-europe/ (accessed March 2016).v
UMF Iasi. Master programme. Faculty of Dentistry Iasi. Available online at http://www.umfiasi.ro/Facultati/FACULTATEA%20DE%20MEDICINA%20DENTARA/Educatie/Pagini/Masterate.aspx (accessed July 2015).
UMF Tirgu Mures. Master programme, Faculty of Dentistry Timisoara. Available online at https://www.umftgm.ro/masterat/medicina-dentara.html (accessed July 2015).
UMF Cluj. Master programme, Faculty of Dentistry Cluj. Available online at http://www.meddent.umfcluj.ro/index.php/ro/educatie-stoma-ro/masterat-md-ro (accessed July 2015).
Ministry of Public Health. [Homepage]. Available online at http://www.ms.ro (accessed July 2015).
Petersen P E, Danila I, Delean A et al. Oral health status among schoolchildren in Romania, 1992. Community Dent Oral Epidemiol 1994; 22: 90–93.
Petersen P E, Rusu M. Oral health status of Romanian schoolchildren – national survey 2000.Copenhagen: WHO Regional Office for Europe, 2002.
Baciu D, Danila I, Balcos C, Gallagher J E, Bernabe E . Caries experience among Romanian schoolchildren: prevalence and trends 1992–2011. Community Dent Health 2015; 32: 93–97.
International Agency for Research on Cancer (WHO). The Globocan Project. Available online at http://globocan.iarc.fr/Default.aspx (accessed August 2015).
European Comminssion. Eurobarometer 2014. Available online at http://ec.europa.eu/public_opinion/archives/ebs/ebs_429_fact_ro_en.pdf (accessed August 2015).
WHO. Global Health Expediture Database. Health expenditure, public. Available online at http://data.worldbank.org/indicator/SH.XPD.PUBL.ZS/countries/1W?display=default (accessed August 2015).
WHO-Global Health Expenditure Database. Health expenditure per capita. Accessed from. http://data.worldbank.org/indicator/SH.XPD.PCAP/countries/1W?display=default (accessed August 2015).
Amariei C, Eaton K A, Systems for the Provision of Oral Health Care in the Black Sea Countries Part 1: Romania, 2009. Oral Health Dent Manag Black Sea Count 2009; 1: 3–6.
World Health Organization. Regional Office for Europe. Health and Economic Development in South-Eastern Europe. WHO, 2006.
National Institute of Statistics. Life expectancy in Romania. Available online at http://www.insse.ro/cms/files/publicatii/pliante%20statistice/07Speranta%20de%20viata_n.pdf (accessed August 2015).
Campaign “Smile Romania”. Accessed from http://www.zambesteromania.ro on 12 August 2015.
Eurobarometer. Report: Oral Health. 2010. Available online at http://ec.europa.eu/public_opinion/archives/ebs/ebs_330_en.pdf (accessed July 2015).
Author information
Authors and Affiliations
Rights and permissions
About this article

Cite this article
Oancea, R., Amariei, C., Eaton, K. et al. The healthcare system and the provision of oral healthcare in European Union member states: Part 5: Romania. Br Dent J 220, 361–366 (2016). https://doi.org/10.1038/sj.bdj.2016.265
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2016.265
This article is cited by
-
Romanian dilemmas
British Dental Journal (2021)
-
Romanian insight
British Dental Journal (2021)
-
Knowledge, dentist confidence and management of periodontal patients among general dentists from Belarus, Lithuania, Macedonia, Moldova and Romania
BMC Oral Health (2020)
-
The healthcare systems and provision of oral healthcare in European Union member states. Part 10: comparison of systems and with the United Kingdom
British Dental Journal (2019)
