
Abstract
Background/objectives
To investigate outcomes of referrals for suspected angle closure and explore whether anterior segment optical coherence tomography (AS-OCT) can be used to tighten triaging criteria in a glaucoma virtual clinic.
Subjects/methods
Retrospectively collected data. The first audit (04/2018-03/2019) identified referrals for suspected angle closure without other glaucoma-related findings (primary angle closure suspect (PACS) referrals). All patients underwent gonioscopy. The second audit (04-08/2019) identified patients with suspected angle closure in a virtual clinic. Management outcomes were assessed, using gonioscopy as reference standard. The outcomes of the second audit were re-audited after changing the triaging criterion from angle width <10° to iridotrabecular contact (ITC) in ≥1 quadrants on AS-OCT.
Results
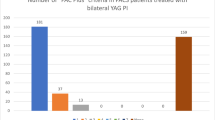
Out of 1754 glaucoma referrals (first audit), 24.6% (431/1754) were PACS referrals. Of these, only 10.7% (42/393) had an occludable angle on gonioscopy, with 97.6% (41/42) being PACS. Of these, 78% (32/41) underwent laser peripheral iridotomy. Out of 137 referrals in the virtual clinic (second audit), 66.4% (91/137) were triaged to the face-to-face clinic. Of these, 31.9% (29/91) were discharged. AS-OCT had positive and negative predictive value of 74.3% (95% confidence intervals (CI) 57.8–86.0) and 82.1% (95% CI 70.0–90.2%), respectively, in detecting ITC in ≥1 quadrants. In the re-audit 45.9% (45/98) of those with suspected angle closure were triaged for gonioscopy, with 24.4% (11/45) of them being discharged.
Conclusion
PACS referrals represent a substantial burden to hospital-based services and their accuracy is low. ITC in ≥1 quadrants on AS-OCT can be useful in triaging those who need further evaluation with gonioscopy.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 18 print issues and online access
$259.00 per year
only $14.39 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
NICE guidance for angle closure (Last revised in February 2023) [Available from: https://cks.nice.org.uk/topics/glaucoma/management/acute-angle-closure-angle-closure-glaucoma/.
Azuara-Blanco A, Burr J, Ramsay C, Cooper D, Foster PJ, Friedman DS, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388:1389–97.
He M, Jiang Y, Huang S, Chang DS, Munoz B, Aung T, et al. Laser peripheral iridotomy for the prevention of angle closure: a single-centre, randomised controlled trial. Lancet. 2019;393:1609–18.
The Royal College of Ophthalmologists. Clinical Guidelines. The Management of Angle-Closure Glaucoma 2022 [Available from: https://www.rcophth.ac.uk/resources-listing/management-of-angle-closure-glaucoma-guideline/.
Simons AS, Vercauteren J, Barbosa-Breda J, Stalmans I. Shared care and virtual clinics for glaucoma in a hospital setting. J Clin Med. 2021;10:4785.
Lawal AK, Rotter T, Kinsman L, Machotta A, Ronellenfitsch U, Scott SD, et al. What is a clinical pathway? Refinement of an operational definition to identify clinical pathway studies for a Cochrane systematic review. BMC Med. 2016;14:35.
Burton MJ, Ramke J, Marques AP, Bourne RRA, Congdon N, Jones I, et al. The Lancet Global Health Commission on Global Eye Health: vision beyond 2020. Lancet Glob Health. 2021;9:e489–e551.
Radhakrishnan S, Rollins AM, Roth JE, Yazdanfar S, Westphal V, Bardenstein DS, et al. Real-time optical coherence tomography of the anterior segment at 1310 nm. Arch Ophthalmol. 2001;119:1179–85.
Van Herick W, Shaffer RN, Schwartz A. Estimation of width of angle of anterior chamber. Incidence and significance of the narrow angle. Am J Ophthalmol. 1969;68:626–9.
Shaffer RN, Schwartz A. Gonioscopy. Surv Ophthalmol. 1957;2:389–409.
Friedman DS. Angle closure and angle closure glaucoma: reports and consensus statements of the 3rd global aigs consensus meeting on angle closure glaucoma: The Hague, The Netherlands: Kugler Publications; 2006.
Becker BSR Diagnosis and Therapy of the Glaucomas: C.V. Mosby; 1965.
Nolan WP, See JL, Chew PT, Friedman DS, Smith SD, Radhakrishnan S, et al. Detection of primary angle closure using anterior segment optical coherence tomography in Asian eyes. Ophthalmology. 2007;114:33–9.
Annoh R, Loo CY, Hogan B, Tan HL, Tang LS, Tatham AJ. Accuracy of detection of patients with narrow angles by community optometrists in Scotland. Ophthalmic Physiol Opt. 2019;39:104–12.
Government GosGTS. https://www.sehd.scot.nhs.uk/pca/PCA2022(O)01.pdf [General ophthalmic services (GOS). The Scottish Government].
Bowling B, Chen SD, Salmon JF. Outcomes of referrals by community optometrists to a hospital glaucoma service. Br J Ophthalmol. 2005;89:1102–4.
Tuck MW, Crick RP. Efficiency of referral for suspected glaucoma. BMJ. 1991;302:998–1000.
Sheldrick JH, Ng C, Austin DJ, Rosenthal AR. An analysis of referral routes and diagnostic accuracy in cases of suspected glaucoma. Ophthalmic Epidemiol. 1994;1:31–9.
Vernon SA, Ghosh G. Do locally agreed guidelines for optometrists concerning the referral of glaucoma suspects influence referral practice? Eye (Lond). 2001;15:458–63.
Theodossiades J, Murdoch I, Cousens S. Glaucoma case finding: a cluster-randomised intervention trial. Eye (Lond). 2004;18:483–90.
Lockwood AJ, Kirwan JF, Ashleigh Z. Optometrists referrals for glaucoma assessment: a prospective survey of clinical data and outcomes. Eye (Lond). 2010;24:1515–9.
Shah S, Murdoch IE. NICE - impact on glaucoma case detection. Ophthalmic Physiol Opt. 2011;31:339–42.
Founti P, Topouzis F, Holló G, Cvenkel B, Iester M, Haidich AB, et al. Prospective study of glaucoma referrals across Europe: are we using resources wisely? Br J Ophthalmol. 2018;102:329–37.
Khan S, Clarke J, Kotecha A. Comparison of optometrist glaucoma referrals against published guidelines. Ophthalmic Physiol Opt. 2012;32:472–7.
Landgren K, Peters D. A prospective study on effectiveness of elevated intraocular pressure as a criterion for glaucoma referrals by optometric practitioners in Sweden. Acta Ophthalmol. 2021;99:e1098–e105.
Nilsson AG, Peters D. Effectiveness of elevated intraocular pressure as a criterion for glaucoma referral after 6 years of follow-up. Clin Ophthalmol. 2021;15:3041–9.
Huang J, Yapp M, Hennessy MP, Ly A, Masselos K, Agar A, et al. Impact of referral refinement on management of glaucoma suspects in Australia. Clin Exp Optom. 2020;103:675–83.
The College of Optometrists. Clinical Management Guidelines [Available from: https://www.college-optometrists.org/clinical-guidance/clinical-management-guidelines/primaryangleclosure_primaryangleclosureglaucoma_pa.
The Scottish Intercollegiate Guidelines Network (SIGN) 2015 [Available from: https://www.sign.ac.uk/our-guidelines/glaucoma-referral-and-safe-discharge/.
Jindal A, Ctori I, Virgili G, Lucenteforte E, Lawrenson JG. Non-contact tests for identifying people at risk of primary angle closure glaucoma. Cochrane Database Syst Rev. 2020;5:Cd012947.
Azuara-Blanco A. Cochrane corner: non-contact tests for identifying people at risk of primary angle closure glaucoma. Eye (Lond). 2021;35:1048–9.
Foster PJ, Devereux JG, Alsbirk PH, Lee PS, Uranchimeg D, Machin D, et al. Detection of gonioscopically occludable angles and primary angle closure glaucoma by estimation of limbal chamber depth in Asians: modified grading scheme. Br J Ophthalmol. 2000;84:186–92.
Day AC, Baio G, Gazzard G, Bunce C, Azuara-Blanco A, Munoz B, et al. The prevalence of primary angle closure glaucoma in European derived populations: a systematic review. Br J Ophthalmol. 2012;96:1162–7.
Porporato N, Baskaran M, Tun TA, Sultana R, Tan M, Quah JH, et al. Understanding diagnostic disagreement in angle closure assessment between anterior segment optical coherence tomography and gonioscopy. Br J Ophthalmol. 2020;104:795–9.
Radhakrishnan S, Chen PP, Junk AK, Nouri-Mahdavi K, Chen TC. Laser Peripheral Iridotomy in Primary Angle Closure: A Report by the American Academy of Ophthalmology. Ophthalmology. 2018;125:1110–20.
The Royal College of Ophthalmologists. The Way Forward 2017 [Available from: https://www.rcophth.ac.uk/standardspublications-research/the-way-forward/.
Sakata LM, Lavanya R, Friedman DS, Aung HT, Seah SK, Foster PJ, et al. Assessment of the scleral spur in anterior segment optical coherence tomography images. Arch Ophthalmol. 2008;126:181–5.
Wong HT, Chua JL, Sakata LM, Wong MH, Aung HT, Aung T. Comparison of slitlamp optical coherence tomography and scanning peripheral anterior chamber depth analyzer to evaluate angle closure in Asian eyes. Arch Ophthalmol. 2009;127:599–603.
Sakata LM, Lavanya R, Friedman DS, Aung HT, Gao H, Kumar RS, et al. Comparison of gonioscopy and anterior segment ocular coherence tomography in detecting angle closure in different quadrants of the anterior chamber angle. Ophthalmology. 2008;115:769–74.
Narayanaswamy A, Sakata LM, He M-G, Friedman DS, Chan Y-H, Lavanya R, et al. Diagnostic performance of anterior chamber angle measurements for detecting eyes with narrow angles: an anterior segment OCT study. Arch Ophthalmol. 2010;128:1321–7.
European Glaucoma Society. Terminology and Guidelines for Glaucoma. 5th Edition: PubliComm, Savona, Italy 2020.
Gedde SJ, Chen PP, Muir KW, Vinod K, Lind JT, Wright MM, et al. Primary angle-closure disease preferred practice pattern®. Ophthalmology. 2021;128:P30–70.
Asia Pacific Glaucoma Society. Glaucoma Guidelines. 3rd Edition. Amsterdam, The Netherlands: Kugler Publications; 2016.
Ho YF, Hu FC, Lee PI. The advantages and challenges of using real-world data for patient care. Clin Transl Sci. 2020;13:4–7.
US Food and Drug Administration. Real-World Evidence 2022 [Available from: https://www.fda.gov/science-research/science-and-research-special-topics/real-world-evidence.
Author information
Authors and Affiliations
Contributions
Design of the study: PF, WN. Data acquisition: AN, AR, NN, SBT. Data analysis: PF, WN, AN, AR, NN, SBT. Interpretation of data: PF, AN, AR, NN, SBT, RT, AS, AM, WN. Drafting the work: PF, WN. Revising the work critically for important intellectual content: PF, AN, AR, NN, SBT, RT, AS, AM, WN Final approval of the version to be published: PF, AN, AR, NN, SBT, RT, AS, AM, WN. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: PF, AN, AR, NN, SBT, RT, AS, AM, WN.
Corresponding author
Ethics declarations
Competing interests
PF and WN received honorarium from Thea. The authors declare no competing financial interests in relation to the work described.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Founti, P., Narayan, A., Raja, A. et al. Outcomes of newly referred patients with suspected angle closure: do we need to redefine the clinical pathways?. Eye 38, 514–519 (2024). https://doi.org/10.1038/s41433-023-02713-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-023-02713-7
