
Abstract
Long-term parenteral nutrition (PN) may induce bone complications. Tridimensional bone imaging techniques such as high-resolution peripheral quantitative computed tomography (HR-pQCT) allow the assessment of both compartmental volumetric densities and microarchitecture. Our aim was to evaluate these parameters in children and teenagers receiving long-term PN. This cross-sectional, case–control study included children older than 9 years undergoing PN for at least 2 years. They were age-, gender- and puberty-matched with healthy controls (1:2). Evaluation included biological assessment of bone metabolism (serum calcium, phosphate, and albumin; urinary calcium and creatinine; 25-OH vitamin D, osteocalcin and PTH), dual X-ray absorptiometry (DXA) and HR-pQCT at the ultradistal tibia and radius. Results are presented as median [range]. Eleven patients (3 girls) with a median age of 16 [9–19] years were included. Bone parameters assessed by HR-pQCT at the ultradistal radius and tibia were similar in patients and controls. Parathyroid hormone (PTH) levels were higher (14 [7–115] vs 16 [12–27]) and osteocalcin levels were lower (44 [15–65] vs 65 [38–142]) in patients than in controls, although within the normal range. Conclusions: there were no differences for compartmental bone densities and microarchitecture in patients undergoing chronic PN. Further longitudinal studies are required to confirm these quite reassuring preliminary results.
Similar content being viewed by others

Introduction
Long-term parenteral nutrition (PN) is the most efficient way to prevent malnutrition in patients with severe intestinal failure (IF). However, PN may induce complications such as bone impairment, also called PN-associated metabolic bone disease (PN-MBD)1,2,3,4,5,6. PN-MBD was first described in 19805,7. It is associated with osteoporosis and impaired mineralization8. Very few data are available on its exact prevalence, but it is estimated to range from 40 to 90% in adults and from 25 to 80% in children and teenagers9,10,11,12.
PN-MBD may be associated with metabolic abnormalities such as hypercalcemia, hypercalciuria, acidosis and hypophosphatemia. Even though the pathophysiology of PN-MBD remains to be fully determined, different parameters are nevertheless known to increase the risk of PN-MBD, namely inadequate PN composition (calcium, phosphate, and lactate), the presence of an underlying inflammatory disease, and treatment with corticosteroids.
Teenagers are particularly at risk for PN-MBD because of growth and acquisition of 25% of bone mass during puberty (and 90% over the first two decades of life). However, there are very limited data on long-term bone impairment in children and teenagers undergoing long-term PN.
Dual X ray Absorptiometry (DXA) is the most used technique to assess bone quantity; it is recommended to assess the longitudinal bone health for children at risk13. Total bone mineral content (TBMC) must be used for bone assessment according to these recommendations, expressing z scores with reference data based at least on age and gender. However, DXA has some technical limitations, especially in growing children and teenagers13,14,15: (i) DXA measures areal density rather than volumetric density that can be modified by growth; (ii) it is unable to evaluate separately trabecular and cortical bone that are sometimes impaired independently; and (iii) DXA cannot determine bone microarchitecture, which is a major determinant of the risk of bone fracture16.
Therefore, innovative tridimensional and non-invasive bone imaging techniques have been developed in the early 2000s, such as high-resolution peripheral quantitative computed tomography (HR-pQCT), allowing the assessment of both compartmental (i.e. total, cortical and trabecular) volumetric densities and trabecular microarchitecture in vivo14,17,18,19,20. This improved bone assessment, especially in children and teenagers whose bones continually grow in mass, size, and shape. To our knowledge, HR-pQCT has never been studied in pediatric patients receiving long-term PN.
We hypothesized that children and teenagers receiving chronic PN may display significant bone microarchitecture differences compared with controls matched for age, gender and pubertal status.
The objectives of this pilot study were (1) to determine the density and bone microarchitecture in children and teenagers receiving long-term PN compared to healthy controls, using HR-pQCT; (2) to compare HR-pQCT results to DXA measurements; and (3) to evaluate the biological markers of bone metabolism.
Patients and methods
This cross-sectional, comparative case-controlled pilot study was performed in the home parenteral nutrition pediatric unit of a university pediatric hospital between March 2014 and June 2015.
Patients
Inclusion criteria were children receiving home PN for more than 2 years for intestinal failure, which seems a sufficiently long period to evaluate the impact of PN on bone metabolism; older than 9 years of age due to technical limitations of HR-pQCT (need to have a perfectly still child), and with regular follow-up in a university HPN center. Exclusion criteria were congenital bone diseases (2 patients with McKusick syndrome) and corticosteroid use for more than one month during the 6 previous months (1 patients with rheumatologic inflammatory disease).
For each assessment, the patient’s anthropometric data were collected: birth term, birth height and weight, gender, weight, height, BMI, and Tanner status. For the same patient, all anthropometric measurements were performed by the same operator during follow-up appointments in a standardized manner: for height, with a wall height chart with increments of 0.5 cm; for weight, with a calibrated scale with increments of the nearest 0.1 kg. The Z-scores were calculated for each value according to national data references21. Tibia length was measured, the knee flexed at 90%, from the proximal margin of the medial malleolus to the proximal border of the medial tibial condyle (manually located) with a tape measure by the same trained operator. For each patient, IF characteristics and bone complication histories were obtained from medical files: IF etiology and intestinal residual length with or without ileocecal valve, fractures and bone pain.
PN was formulated according to the child’s individual needs.
The study was approved by a local independent ethics committee (CPP Lyon Sud-Est II, ID-RCB2013-A01245-40), parental informed consent was obtained for each pediatric patient, and all methods were performed in accordance with the relevant guidelines and regulations. The study was registered in Clinical Trial (NCT02368496; 23 February 2015).
Healthy volunteers
Each patient undergoing PN participating in this study was matched by gender, age and pubertal status (Tanner stage) to two controls recruited concomitantly and locally in the VITADOS cohort of healthy children (NCT 01832623; 16 April 2013), as previously published22.
Biological data
All biological analyses were performed in the same laboratory, immediately after blood sample, in the morning with fasted patients. Usually, in children or adolescent with long-term PN, the frequency of standard biological follow-up is each 3 month when patients are stable. Serum calcium, phosphate, albumin, urinary calcium and creatinine were measured by routine laboratory methods. Intact parathyroid hormone was measured with a second generation assay (Roche Elecsys, Roche Diagnosis, Mannheim, Germany), 25-OH vitamin D with a radio-immunological technique (DiaSorin Assay, DiaSorin Diagnosis, Saluggia, USA), and serum NMID osteocalcin (N-terminal mid fragment of osteocalcin) with immune-chemiluminescence (LIAISON XL, DiaSorin Diagnosis, Saluggia, USA). Glomerular filtration was calculated with the new equation published before23.
HR-pQCT
HR-pQCT measurements were performed at the non-dominant limb unless there was a history of fracture, as previously reported by our team in children24. Volumetric bone mineral density (vBMD) and bone microstructure were measured at the distal radius and tibia using a HR-pQCT device (XtremeCT, SCANCO Medical AG, Brüttisellen, Switzerland) that acquires a stack of 110 parallel CT slices with an isotropic voxel size of 82 µm. A scout-view (dorsal–palmar radiography) allowed positioning of a reference line at the endplate. The first slice of the ROI was set at 22.5 mm of the reference line at the ultra-distal tibia and 9.5 mm at the ultra-distal radius, which extended proximally on 110 slices, i.e., 9.02 mm in the axial direction, as previously described. The following imaging settings were used: effective energy = 60 kVp, X-ray tube current = 900µA, integration time = 100 ms. The 126 mm field of view was reconstructed on a 1536 × 1536 matrix, yielding 82 µm isotropic voxels. The total scan time was 2.8 min with an equivalent dose of approximately 3 μSv. Attenuation data were converted to equivalent hydroxyapatite (HA) densities. A phantom was scanned daily for quality control.
For the standard analysis, a trained operator generates semi-automatic contours around the periosteal surface in scans without motion artifact; the entire volume of interest is thereafter automatically separated into a cortical and trabecular region. The outcome variables included total area (Tt.Ar, mm2), volumetric bone density (mg HA/cm3) for total (Tt.BMD), trabecular (Tb.BMD), and cortical (Ct.BMD) compartments; cortical thickness (Ct.Th, µm); and trabecular number (Tb.N, mm-1), thickness (Tb.Th, µm), separation (Tb.Sp, µm), and intra-individual distribution of separation (Tb.Sp.SD, µm). In clinical practice, the higher the trabecular number and thickness, the better the trabecular status; the lower the trabecular separation and distribution, the better the trabecular status.
DXA: dual X-ray absorptiometry
Whole body DXA and spine DXA were performed with a fan beam (Hologic Discovery W, Hologic, Inc., Bedford, MA) in the array using standard positioning techniques. We performed the standard pediatric protocol of total body less head. The Lumbar spine measurements included L1-L4. The DXA whole body and spine scans were analyzed to generate measures of whole body projected bone area (cm2), bone mineral content (BMC) (g) and bone mineral density (BMD) (g/cm2). Lean mass (kg) and fat mass (FM) (kg) were obtained from the whole body DXA scan excluding the skull.
Statistical analysis
Statistical analyses were performed using the SPSS Software. All eligible patients were included. Comparisons between patients and controls were performed using the nonparametric Wilcoxon signed rank test since the number of patients was low. Correlations between density, microarchitectural and biological parameters were computed with the Spearman bivariate analysis. All statistical tests were performed at the two-sided 0.05 level of significance. Data are presented as median, minimum and maximum: med [min–max].
Results
Subjects characteristics
We included 11 patients and 22 controls. Anthropometric and clinical data for patients and controls are summarized in Table 1.
The median age of initiating PN was 17 (0–150) months, and this nutritional support was given for a median of 10.3 (6.4–18.3) years at the time of this study.
All patients receiving long-term PN had intestinal failure; etiologies are indicated in Table 1.
Two patients at the time of examination had withdrawn PN since 4 months and 5 months respectively. Calories in parenteral nutrition represented a median intake of 77 (40–190) % of recommended dietary allowances. All patients also had oral supplementation: 100 000 UI of vitamin D3 each 3 months. Median vitamin D3 intake in PN was 220 (0–250) UI/day. Table 2 summarizes the main PN parameters applied to this cohort.
Three patients had also enteral nutrition during PN or during nights without PN.
Four patients and one control had history of long bone fracture, none had a vertebral fracture and none had more than two fractures. All were traumatic fractures.
Biological parameters
Biological parameters for patients and controls are also summarized in Table 1. Nutritional biological parameters (albumin, prealbumin, urea, creatinin and eGFR according to the recent equation) were normal in the 2 groups; however compared to controls, PN patients displayed lower median albumin levels (84% of controls; p = 0.015) but higher prealbumin (127% of controls; p = 0.035) and urea levels (114% of controls; p = 0.048). Parameters of calcium/phosphate and bone metabolism (calcium, phosphate, urinary calcium to creatinine ratio, 25 hydroxy-vitamin D and total alkaline phosphatase) were similar between the two groups. However, PN patients displayed higher but normal PTH (256% of controls; p = 0.003) and lower but normal osteocalcin plasmatic levels (67% of controls; p = 0.005), as compared to controls.
HR-pQCT
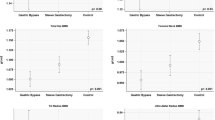
At the radius, no significant differences were observed between controls and PN patients, as illustrated in Table 3. However at the tibia, PN children displayed a lower trabecular area compared to controls (470 [124–675] vs 606.5 [369–897] µm2, p = 0.003).
DXA and body composition
Body composition data are summarized in Tables 3 and 4. BMC was similar to controls; only the BMD of the whole body was significantly lower in patients (0.81 [0.54–0.96] vs 0.92 [0.66–1.35], p = 0.039). In terms of body composition, the global distribution was similar between patients and healthy patients. However patients differed according the gynoid lean and total mass distribution. The android-gynoid ratios and the BMI were similar to the controls.
Discussion
This pilot prospective study is the first to evaluate bone microarchitecture with HR-pQCT in pediatric patients undergoing long-term PN in comparison to healthy controls. The main results are: (1) reassuring results for bone quality and body composition evaluated by both HR-pQCT (with similar densities and microarchitecture between PN patients and controls) and DXA (with BMC similar to controls); and (2) higher but normal PTH levels despite correct vitamin D levels, with lower but normal osteocalcin levels in PN patients as compared to controls.
PN-associated metabolic bone disease
The main previous studies that have described bone diseases in patients receiving home PN were adult studies5,8,11. The first pediatric study was published in 201025. Of note, 83% of these patients had bone mineral deficiency and 17% had fractures. Different studies evaluated longitudinal evolution and predictive factors, including intestinal failure-related factors and parenteral nutrition-related factors15,25,26,27. Risk factors identified were: (1) the etiology of intestinal failure: patients with a small bowel syndrome were more at risk for bone disease; (2) the duration of PN was correlated to lower lumbar BMD; (3) others factors such as the small bowel length and the presence of the ileocecal valve did not predict BMD.
Compared to previous pediatric studies, our cohort had less PN-MBD (only 2 (18%) patients had a whole body BMC ≤ − 2 DS). Several reasons may explain this discrepancy: the etiologies are different since we excluded patients with inflammatory bowel disease and patients having received steroid therapy for more than 1 month during the 6 previous months. These etiologies differ from other studies describing lower bone mineral density in patients on long-term PN which may include inflammatory bowel disease4,8,9,11. We can also hypothesize that the treatment and patient care were effective in preventing bone deterioration.
A significant fracture history is defined by either one or more vertebral crush fractures, two or more long bone fractures by 10 years of age, or three or more fractures by 19 years of age12. The clinical bone history of our patients indicates that four patients had a past of bone fracture, and only one control subject. However, as noted below, radiological exams (HR-pQCT and DXA) were not significantly different between the two groups. It seems unlikely that all radiological measurements are ineffective to identify the risk of bone fracture, and we face here one of the main limitations of this cohort namely its limited size.
Determination of the density and bone microarchitecture in children and teenagers with long-term PN.
Compared to DXA, the main objective of HR-pQCT is to evaluate microarchitectural composition. Low trabecular area and high trabecular separation are associated with an increased risk of osteoporosis. This profile associated with bone fragility is described only at the ultra-distal tibia of our patients, and only with a small difference. However, there are no significant differences in cortical parameters that are involved more in bone strength than trabecular ones. Many studies have shown an increased cortical vBMD with age without modifications of trabecular parameter18,28,29. Cortical vBMD measured by HR-pQCT increased with puberty in both genders28. Therefore, this small difference reported only at the ultra-distal tibia of patients should have only a minor effect if any on bone solidity.
Comparison of HR-pQCT results to DXA measurements
Our study seems to indicate very mild differences of mineral status with both radiological techniques when compared patient to healthy controls. On one hand, HR-pQCT indicates no difference in BMD but only minor trabecular changes at the tibia; on the other hand DXA indicates no alteration of the main parameters (namely spine BMD, BMC or whole body BMC that correspond to the recommended measure sites in pediatrics)30.
BMD had divergent results with the two radiological techniques: HR-pQCT measured similar total volumetric BMD in patients and controls. In contrast, DXA showed a significant lower whole body subtotal BMD in patients. This may suggest that (1) inherent differences between the radiological techniques (HR-pQCT versus DEXA); (2) BMD of the ultra-distal radius and tibia do not reflect whole body BMD, but previous studies have found DXA spine and hip scans do correlate with HR-pQCT radius and tibia scans; (3) HR-pQCT and DXA evaluate bone composition differently; (4) our patients were smaller than controls but had a similar BMI. That could explain a lower BMD with DXA. DXA relies on areal density rather than volumetric density that can be modified by growth. Therefore, the risk of underestimating BMD in small children and overestimating BMD in tall children is well known13,31.
Evaluation of the biological markers of bone metabolism
Very few pediatric studies accurately assessed the biological markers of bone metabolism in PN. We did not find biological abnormalities in this study for the markers of bone metabolism; however, as compared to controls, our patients displayed different levels of PTH and osteocalcin that however both remained within the normal range.
Indeed, patients displayed a relative hyperparathyroidism: PTH levels were within the normal range, but significantly higher in patients compared to controls. Hyperparathyroidism in patients on long-term PN has been previously described26,32. A relationship between hyperparathyroidism and bone remodeling was also previously described in adults33,34. In our patients, this higher level of PTH is not explained by a lower vitamin D level, which is similar to healthy controls. Based on international recommendations, a partial deficiency could be considered in patients and controls since vitamin D levels should be higher than 75 nmol/L35. The recommendation for parenteral vitamin D intakes are 400 UI/day36. Our patients received only a median intake of 268 ± 0.87 UI/day in perfusion, but also an oral supplementation of vitamin D every 3 months. Therefore, intestinal malabsorption could explain their low plasmatic level of vitamin D; this result should encourage increasing oral doses and closely monitoring plasmatic vitamin D.
Low calcemia and high phosphoremia could explain a higher PTH. This hormone increases calcium levels and decreases phosphate levels, through a stimulation of 1–25 OH2 vitamin D synthesis and further activation of intestinal calcium absorption, through a stimulation of tubular calcium reabsorption and through an inhibition of the apical expression of the sodium/phosphate transporters Npt2 thus inducing phosphaturia. Last, PTH also has biphasic effects on bone, depending on the levels of PTH and its pulsatility. In our patients, calcium and phosphate parenteral intakes are within the range of the recommendations Calcium 0.35 for 0.25–0.4 mmol/kg/day and phosphate 0.6 for 0.2 to 0.7 mmol/kg/day, whereas the rates of calcemia and phosphatemia were similar in the two groups37. Unfortunately, we do not have urinary calcium and phosphate levels for all patients to evaluate tubular reabsorption. However, the Ca/creat urinary ratio was normal and not different between patients and controls.
Finally, an acid–base imbalance could also increase PTH levels. Indeed, metabolic acidosis rapidly inhibits the CaSR that causes PTH release and relative hyperparathyroidism. Acid–base balance was not specifically studied in this cohort, even if PN patients displayed significant lower plasma bicarbonate concentrations in comparison to controls. However, the values are normal and the difference does not seem clinically relevant.
Osteocalcin
Patients had a significantly lower osteocalcin levels than controls. Osteocalcin is produced by differentiated osteoblasts. Furthermore, non-carboxylated osteocalcin regulates glucose homeostasis by increasing insulin secretion and decreasing insulin resistance.
Osteocalcin level is influenced by different parameters: (1) gender: higher in women; (2) age with a decrease with age in both men and women, and especially during puberty38; (3) physical activity: higher after a run. As our patients are gender- and age-matched with controls, variations of osteocalcin could indicate an impaired glucose metabolism38,39,40. Unfortunately, we do not have the parameters to evaluate this hypothesis such as, for example, the Homeostasis Model Assessment (HOMA) scale of insulin resistance (insulin (mUI/L) × glucose (mmol/L)/22.5)41,42,43. It would be interesting for a future study to collect insulin and glucose levels in these patients.
Several limitations of this study may be highlighted. It is a monocentric study with a small cohort. However, this study was designed as a pilot study, and children receiving long-term PN are rare. Another limitation in the interpretation of results is the significant difference observed in height and body weight between patients and controls, likely explaining the lower trabecular area observed at the weight-bearing tibia in PN patients. Body size differences alone could account for any discrepancies between the clinical and healthy groups, an adjustment for height between patients and controls would ideally be useful. Even though we selected the smallest subjects among the controls (after matching for gender, age and puberty), it was impossible to adjust for height given the difference of height between controls and patients. However, odd differences in height between groups is little, and limb length is similar between the 2 groups; therefore we believe that these two limitations are not crucial in view of the observed results, namely the absence of significant differences in bone status between controls and PN patients28,44,45.
Conclusion and perspectives
This first study evaluating microarchitecture in children receiving long-term PN provides quite reassuring results: the innovative imaging technique HR-pQCT did not find any deterioration of bone outcomes in our cohort after more than 10 years of PN. However, the small sample size requires caution in interpretation. Further longitudinal studies, with larger cohorts, are required to confirm these data and to determine if such techniques could help physicians improve the therapeutic management of children receiving long-term PN.
References
Knafelz, D. et al. Complications of home parenteral nutrition in a large pediatric series. Transplant. Proc. 35(8), 3050–3051 (2003).
Colomb, V. et al. Long-term outcome of children receiving home parenteral nutrition: A 20-year single-center experience in 302 patients. J. Pediatr. Gastroenterol. Nutr. 44(3), 347–353 (2007).
Buchman, A. L. & Moukarzel, A. Metabolic bone disease associated with total parenteral nutrition. Clin. Nutr. Edinb. Scotl. 19(4), 217–231 (2000).
Pironi, L. et al. Prevalence of bone disease in patients on home parenteral nutrition. Clin. Nutr. Edinb. Scotl. 21(4), 289–296 (2002).
Klein, G. L. et al. Bone disease associated with total parenteral nutrition. Lancet Lond. Engl. 2(8203), 1041–1044 (1980).
Hurley, D. L. & McMahon, M. M. Long-term parenteral nutrition and metabolic bone disease. Endocrinol. Metab. Clin. North Am. 19(1), 113–131 (1990).
Shike, M. et al. Metabolic bone disease in patients receiving long-term total parenteral nutrition. Ann. Intern. Med. 92(3), 343–350 (1980).
Pironi, L. et al. Bone mineral density in patients on home parenteral nutrition: A follow-up study. Clin. Nutr. Edinb. Scotl. 23(6), 1288–1302 (2004).
Haderslev, K. V., Tjellesen, L., Haderslev, P. H. & Staun, M. Assessment of the longitudinal changes in bone mineral density in patients receiving home parenteral nutrition. JPEN 28(5), 289–294 (2004).
Neelis, E. et al. Bone health of children with intestinal failure measured by dual energy X-ray absorptiometry and digital X-ray radiogrammetry. Clin. Nutr. Edinb. Scotl. 37(2), 687–694 (2018).
Raman, M. et al. Metabolic bone disease in patients receiving home parenteral nutrition: A Canadian study and review. JPEN 30(6), 492–496 (2006).
Bishop, N. et al. Fracture prediction and the definition of osteoporosis in children and adolescents: The ISCD 2013 Pediatric Official Positions. J. Clin. Densitom Off. J. Int. Soc. Clin. Densitom. 17(2), 275–280 (2014).
Binkovitz, L. A., Henwood, M. J. & Sparke, P. Pediatric DXA: Technique, interpretation and clinical applications. Pediatr. Radiol. 38(Suppl 2), S227-239 (2008).
Bacchetta, J. et al. Bone assessment in children with chronic kidney disease: Data from two new bone imaging techniques in a single-center pilot study. Pediatr. Nephrol. Berl. Ger. 26(4), 587–595 (2011).
Poinsot, P. et al. Longitudinal bone mineralization assessment in children treated with long-term parenteral nutrition for severe intestinal failure. JPEN 42(3), 613–622 (2018).
Weber, L. T. & Mehls, O. Limitations of dual x-ray absorptiometry in children with chronic kidney disease. Pediatr. Nephrol. Berl. Ger. 25(1), 3–5 (2010).
Bacchetta, J. et al. Bone metabolism in oxalosis: A single-center study using new imaging techniques and biomarkers. Pediatr. Nephrol. Berl. Ger. 25(6), 1081–1089 (2010).
Bacchetta, J. et al. Assessment of bone microarchitecture in chronic kidney disease: A comparison of 2D bone texture analysis and high-resolution peripheral quantitative computed tomography at the radius and tibia. Calcif. Tissue Int. 87(5), 385–391 (2010).
Sornay-Rendu, E., Boutroy, S., Duboeuf, F. & Chapurlat, R. D. Bone microarchitecture assessed by HR-pQCT as predictor of fracture risk in postmenopausal women: The OFELY Study. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 32(6), 1243–1251 (2017).
Boutroy, S., Bouxsein, M. L., Munoz, F. & Delmas, P. D. In vivo assessment of trabecular bone microarchitecture by high-resolution peripheral quantitative computed tomography. J. Clin. Endocrinol. Metab. 90(12), 6508–6515 (2005).
Rolland-Cachera, M. F. et al. Body Mass Index variations: Centiles from birth to 87 years. Eur. J. Clin. Nutr. 45(1), 13–21 (1991).
Bacchetta, J. et al. Assessment of mineral and bone biomarkers highlights a high frequency of hypercalciuria in asymptomatic healthy teenagers. Acta Paediatr Oslo Nor 1992 108(12), 2253–2260 (2019).
Schwartz, G. J. et al. New equations to estimate GFR in children with CKD. JASN 20(3), 629–637 (2009).
Vierge, M. et al. Pediatric bone evaluation with HR-pQCT: A comparison between standard and height-adjusted positioning protocols in a cohort of teenagers with chronic kidney disease. Arch. Pediatr. Organe Off. Soc. Francaise Pediatr. 26(3), 151–157 (2019).
Diamanti, A. et al. How does long-term parenteral nutrition impact the bone mineral status of children with intestinal failure?. J. Bone Miner. Metab. 28(3), 351–358 (2010).
Demehri, F. R. et al. Pediatric intestinal failure: Predictors of metabolic bone disease. J. Pediatr. Surg. 50(6), 958–962 (2015).
Khan, F. A. et al. Metabolic bone disease in pediatric intestinal failure patients: prevalence and risk factors. J. Pediatr. Surg. 50(1), 136–139 (2015).
Kirmani, S. et al. Bone structure at the distal radius during adolescent growth. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 24(6), 1033–1042 (2009).
Neu, C. M., Manz, F., Rauch, F., Merkel, A. & Schoenau, E. Bone densities and bone size at the distal radius in healthy children and adolescents: A study using peripheral quantitative computed tomography. Bone 28(2), 227–232 (2001).
Kalkwarf, H. J. et al. Bone densitometry in infants and young children: The 2013 ISCD Pediatric Official Positions. J. Clin. Densitom Off. J. Int. Soc. Clin. Densitom. 17(2), 243–257 (2014).
Helba, M. & Binkovitz, L. A. Pediatric body composition analysis with dual-energy X-ray absorptiometry. Pediatr. Radiol. 39(7), 647–656 (2009).
Mutanen, A., Mäkitie, O. & Pakarinen, M. P. Risk of metabolic bone disease is increased both during and after weaning off parenteral nutrition in pediatric intestinal failure. Horm. Res. Paediatr. 79(4), 227–235 (2013).
Arabi, A., Baddoura, R., El-Rassi, R. & El-Hajj, F. G. PTH level but not 25 (OH) vitamin D level predicts bone loss rates in the elderly. Osteoporos Int. J. Establ. Result Coop. Eur. Found Osteoporos Natl. Osteoporos Found USA 23(3), 971–980 (2012).
Rejnmark, L., Vestergaard, P., Brot, C. & Mosekilde, L. Increased fracture risk in normocalcemic postmenopausal women with high parathyroid hormone levels: A 16-year follow-up study. Calcif. Tissue Int. 88(3), 238–245 (2011).
Holick, M. F. et al. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 96(7), 1911–1930 (2011).
Bronsky, J., Campoy, C., Braegger, C. & ESPGHAN/ESPEN/ESPR/CSPEN working group on pediatric parenteral nutrition. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Vitamins. Clin. Nutr. Edinb. Scotl. 37(6 Pt B), 2366–78 (2018).
Mihatsch, W. et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Calcium, phosphorus and magnesium. Clin. Nutr. Edinb. Scotl. 37(6 Pt B), 2360–2365 (2018).
Karsenty, G. Update on the biology of osteocalcin. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 23(10), 1270–1274 (2017).
Confavreux, C. Physiologie intégrative du métabolisme énergétique, de l’os et de la fertilité: rôle de l’ostéocalcine et des hormones sexuelles. Disponible sur: https://tel.archives-ouvertes.fr/tel-00864174/document. (2012).
Mera, P. et al. Osteocalcin signaling in myofibers is necessary and sufficient for optimum adaptation to exercise. Cell Metab. 25(1), 218 (2017).
Lienhardt, A. et al. Insulin secretion and sensitivity in children on cyclic total parenteral nutrition. JPEN 22(6), 382–386 (1998).
Confavreux, C. B. Bone: from a reservoir of minerals to a regulator of energy metabolism. Kidney Int. Suppl. 121, S14-19 (2011).
Chapurlat, R. D. & Confavreux, C. B. Novel biological markers of bone: from bone metabolism to bone physiology. Rheumatol. Oxf. Engl. 55(10), 1714–1725 (2016).
MacNeil, J. A. & Boyd, S. K. Accuracy of high-resolution peripheral quantitative computed tomography for measurement of bone quality. Med. Eng. Phys. 29(10), 1096–1105 (2007).
MacNeil, J. A. & Boyd, S. K. Load distribution and the predictive power of morphological indices in the distal radius and tibia by high resolution peripheral quantitative computed tomography. Bone 41(1), 129–137 (2007).
Funding
An institutional funding for the VITADOS cohort was provided by the Programme Hospitalier de Recherche Clinique Inter-régional (PHRCi) (J Bacchetta, 2011). An institutional grant was provided by ALLP for this study.
Author information
Authors and Affiliations
Contributions
T.L., P.P., J.B., N.P.: made substantial contributions to the conception or design of the work; analysis and interpretation of data. L.R. and A.B.: made substantial contributions to the conception and the acquisition of data. I.L.D., S.H., S.M., D.B., C.C., C.B.C., A.L.: drafted the work or revised it critically for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Louazon, T., Poinsot, P., Restier, L. et al. A prospective case–control pilot study to evaluate bone microarchitecture in children and teenagers on long-term parenteral nutrition using HR-pQCT. Sci Rep 11, 9151 (2021). https://doi.org/10.1038/s41598-021-88366-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-88366-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
